
Jagoda Misniakiewicz, PharmD
Scientific Pharmacy Specialist, Medical College of South Carolina
ONCOLOGY spoke with Jagoda Misniakiewicz, PharmD, in regards to the latest approval of fruquintinib for sufferers with metastatic colorectal most cancers. The dialog centered on the mechanism of motion of the agent and the way it compares with different accessible therapy choices within the house.
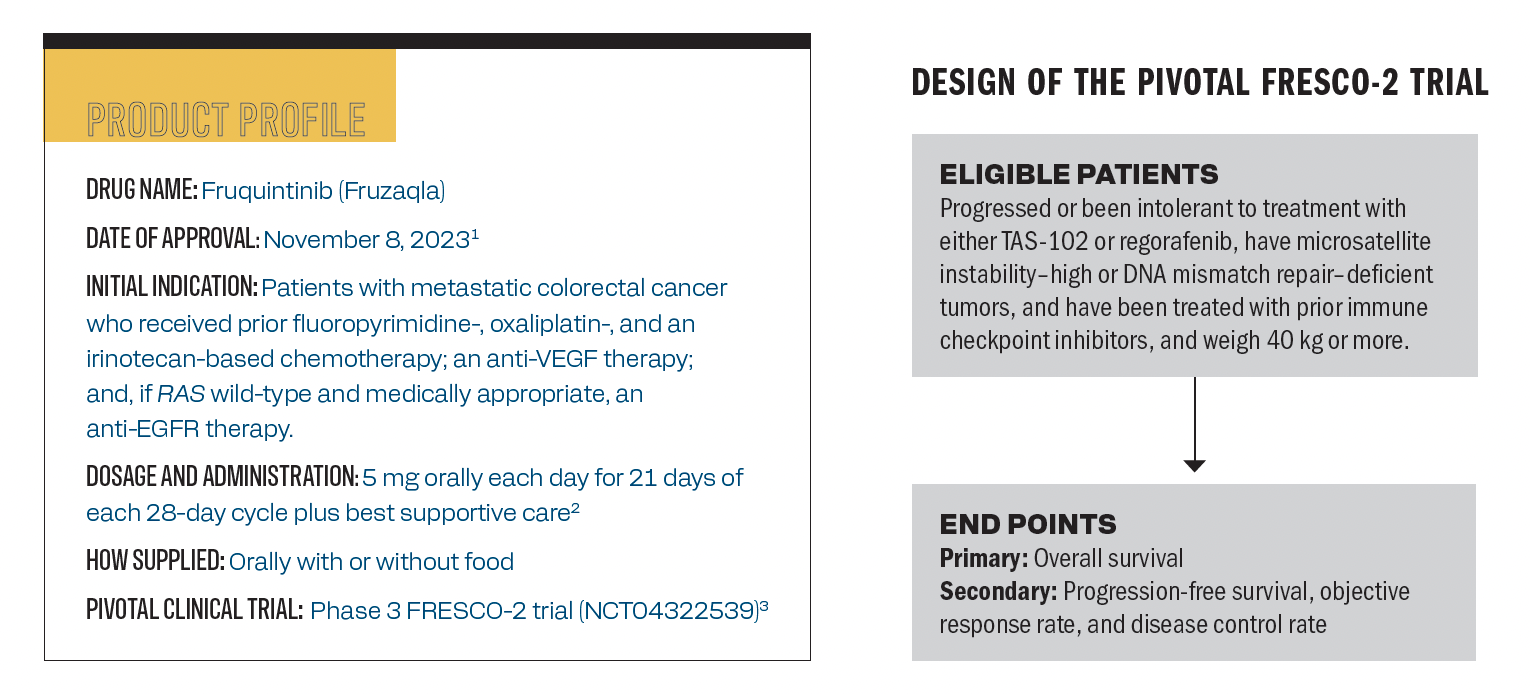
The product profile of fruquintinib.
Q / What’s the mechanism of motion of fruquintinib?
Misniakiewicz / Fruquintinib is a extremely selective and potent oral small-molecule kinase inhibitor of VEGFR-1, -2, and -3, that are key regulators of angiogenesis related to tumor progress and metastasis. Fruquintinib inhibits VEGF-mediated endothelial cell proliferation, tubular formation, VEGF receptor phosphorylation, and tumor progress. Fruquintinib prevents VEGF receptor structural change and dimerization, due to this fact stopping the phosphorylation of the intracellular kinase area that impacts downstream signaling cascades. It straight impacts tumor cell operate by inhibiting new blood vessel progress and leads to vascular regression, normalization, and building. It’s identified that angiogenesis inhibition has been confirmed to be an efficient therapy technique all through the continuum of care in metastatic colorectal most cancers, which led to the [approval] of fruquintinib on this setting. Notably, fruquintinib is a weak inhibitor of RET, FGFR1, and CK kinases, which contributes to lower in tumor progress.
Q / Are there any particular biomarkers or tumor traits that may assist establish sufferers who’re more than likely to learn from fruquintinib?
Misniakiewicz / At present, little is thought in regards to the sample of response to fruquintinib. Within the FRESCO-2 research, the subgroup evaluation confirmed constant outcomes having a profit within the majority of the prespecified subgroups, which had beforehand used TAS-102 [trifluridine, tipiracil, and hydrochloride; Lonsurf], regorafenib [Stivarga], RAS standing, and period of metastatic illness. It confirmed a profit for sufferers who had liver metastases; nevertheless, it could be useful to have extra knowledge on sufferers with lung metastases. Proper now, anybody who has progressed on prior strains of remedy would ideally profit from fruquintinib remedy. There simply must be extra analysis into what’s that particular [patient population] that might present extra profit.
There’s some literature wanting on the efficacy of fruquintinib in sufferers who might have change into proof against bevacizumab [Avastin]. That will be an attention-grabbing inhabitants. Proper now, there aren’t any particular biomarkers or tumor traits that we’re . Most sufferers could be applicable candidates, and we might anticipate them to obtain some profit from fruquintinib remedy. The one exception to that may be sufferers whose [diseases] specific DNA mismatch restore or are microsatellite instability-high [MSI–high], as they’d obtain profit from immunotherapy first, however that most likely isn’t even related presently since fruquintinib is utilized in later settings.
Q / How important was the progression-free survival (PFS) enchancment within the FRESCO-2 trial in contrast with different therapy choices accessible for this inhabitants?
Misniakiewicz / The info that got here out of FRESCO-2 had been thrilling. The forest plot was one thing that everybody was excited by; it confirmed a novel therapy for sufferers with relapsed/refractory colorectal most cancers. Once we take a look at what the PFS is in contrast with the brokers that we might be grouping it with, so regorafenib and TAS-102, there’s a distinction. There aren’t any head-to-head research that however there’s a meta-analysis of 5 medical trials that confirmed no distinction within the efficacy evaluation of total survival and that fruquintinib was superior in PFS in contrast with TAS-102.4 General, I might say that that is important once we take a look at this enchancment, and it does present a promising therapy choice for sufferers with refractory colorectal most cancers.
Q / Have been there any widespread or important adversarial results (AEs) related to this therapy? How do they examine with different brokers within the house?
Misniakiewicz / In keeping with the outcomes from FRESCO-2 and the package deal insert, the commonest AEs of fruquintinib are hypertension and asthenia, which is smart based mostly on its mechanism of motion. It’s comparable with what we might anticipate with different tyrosine kinase inhibitors (TKIs) used for colorectal most cancers and that particular TKI is regorafenib.
Clinically, we will see some variations in AEs. Fatigue has been very important in our sufferers who’re handled with fruquintinib. This can be related to the numerous and fast change of their thyroid operate assessments that we’re seeing. Inside 2 weeks of beginning remedy, sufferers are expressing fast adjustments of their thyroid-stimulating hormone, and that could possibly be contributing to the fatigue that they’re feeling. We’re seeing numerous voice adjustments in hoarseness, which can also be to be anticipated with regorafenib.
Attributable to fruquintinib’s mechanism of motion, one would anticipate AEs associated to the VEGF pathway, so hypertension, proteinuria, bleeding, impaired wound therapeutic, and arterial thromboembolism. These are the identical AEs that I might be looking out for in sufferers handled with regorafenib. The massive distinction that we see is that sufferers handled with regorafenib expertise extra hand-foot syndrome and diarrhea than we’ve seen in sufferers with fruquintinib. Hand-foot syndrome has a excessive incidence within the FRESCO-2 trial; we simply usually are not seeing as a lot as we see in sufferers who’ve been handled with regorafenib.
Q / What are some identified potential resistance mechanisms related to fruquintinib?
Misniakiewicz / The mechanisms of resistance to anti-VEGF therapies usually are not precisely clear. To this point, there are 3 predominant theorized mechanisms that embrace activation of compensatory pathways, redundancy and angiogenic pathways, and MET upregulation and hepatocyte progress issue/c-MET activation. It’s additionally necessary to contemplate that components akin to hypoxia and restricted blood provide can lower drug supply resulting in resistance. Apparently, some methods have been explored to beat these potential resistance mechanisms, together with concentrating on various angiogenic pathways and mixing VEGF targets with PD-1 and MET. It is going to be attention-grabbing to see if fruquintinib has a task in sufferers who might develop resistance to bevacizumab therapies after which differentiate what’s the identified resistance mechanism to bevacizumab. How does that examine with fruquintinib, particularly since we’ll be utilizing it in later strains?
Q / The place do you see this agent headed?
Misniakiewicz / There are at the moment numerous medical trials fruquintinib together with chemotherapy. That might be an avenue to be explored. It’s being studied with chemotherapy in addition to different focused brokers and immunotherapy. Seeing the outcomes of those trials might be attention-grabbing after which seeing it navigate its place within the therapy algorithm may even be attention-grabbing to see what comes of that. I can see fruquintinib making its means into different gastrointestinal malignancies. There’s some research within the gastric most cancers setting, and we’ll see if it would make its means into these pointers within the coming years. Then we’ll see if fruquintinib will proceed to maneuver its means up by way of strains of therapy. The FRESCO-2 trial studied it as a fourth- or fifth-line setting. Proper now, within the pointers, it could possibly be a third-line therapy choice. There are some medical trials fruquintinib together with FOLFOX [leucovorin calcium, fluorouracil, and oxaliplatin] within the first-line setting, so I’m to see what’s going to come of that.
Q / Is there the rest you need to spotlight?
Misniakiewicz / Therapy choices for metastatic colorectal most cancers are restricted, and the approval of fruquintinib will hopefully bridge that hole just a little bit. Oral brokers have modified the panorama of therapy for sufferers with most cancers. Moreover, focused brokers enable us to tailor remedy with the aim of bettering medical outcomes whereas minimizing off-target toxicities. Fruquintinib hopefully permits us to do that and for sufferers with metastatic colorectal most cancers, oral anticancer therapies are an space the place we oncology pharmacists can play a giant function in affected person care. There’s numerous alternatives to assist with AE administration and assist with having the ability to preserve these sufferers on remedy longer, serving to sufferers have entry to therapies, after which having the ability to present sufferers with a remedy the place they don’t want to return into the clinic for lengthy therapy days and making an attempt to optimize their high quality of life. Fruquintinib’s approval has been very thrilling on this house, and I hope to proceed to see nice outcomes with it as we’ve extra sufferers began on it. It’s a giant space for oncology pharmacists to assist handle these toxicities.
References
- Takeda receives U.S. FDA approval of Fruzaqla (fruquintinib) for beforehand handled metastatic colorectal most cancers. Information launch. Takeda. November 8, 2023. Accessed June 6, 2024. https://bit.ly/3SwkD8U
- Fruzaqla. Prescribing data. Takeda; 2023. Accessed June 6, 2024. https://shorturl.at/yMXXP
- Dasari A, Lonardi S, Garcia-Carbonero R, et al; FRESCO-2 Research Investigators. Fruquintinib versus placebo in sufferers with refractory metastatic colorectal most cancers (FRESCO-2): a global, multicentre, randomised, double-blind, part 3 research. Lancet. 2023;402(10395):41-53. doi:10.1016/S0140-6736(23)00772-9
- Chen J, Wang J, Lin H, Peng Y. Comparability of regorafenib, fruquintinib, and TAS-102 in beforehand handled sufferers with metastatic colorectal most cancers: a scientific evaluate and community meta-analysis of 5 medical trials. Med Sci Monit. 2019;25:9179-9191. doi:10.12659/MSM.918411
{kind=link}