
CT screening for lung most cancers may save numerous lives, however low participation charges have led to some eyebrow-raising proposals. Molecular strategies, touted by these with a vested curiosity, promising to pre-screen for eligibility—as a result of who would not need a check to find out in the event that they qualify for the actual check?
Lung most cancers (LC) is a horrible illness that kills greater than 120,000 Individuals yearly, however there’s excellent news. If LC may be detected whereas nonetheless at a small dimension earlier than it has invaded and unfold, it’s curable. And the smaller, the higher, as illustrated by the next information. For instance, the prospect of treatment is 92% when lower than 1 cm. in diameter (IA1) however falls to 73% when past 3cm (IB). After the most cancers has unfold to mediastinal lymph nodes (stage 3) or distant organs (stage 4), the prospect of treatment drops precipitously.
The excellent news is that computerized tomographic screening (CT screening) can detect very small lung cancers under 1 cm in diameter. The unhealthy information is that though CT screening has been coated by personal insurance coverage, Medicare, and Medicaid since 2014, participation amongst these eligible stays very low, and a chance to avoid wasting tens of hundreds of lives is being misplaced.
The Facilities for Medicare and Medicaid Providers (CMS) agreed to offer first-dollar insurance coverage protection for CT screening in 2014 and subsequently has prolonged protection to roughly fourteen million people at elevated threat of lung most cancers, i.e., people who smoke between the ages of 50-77, with greater than twenty pack-years of publicity, and ex-smokers who’ve stop smoking inside the earlier fifteen years.
Regardless of a decade of CMS protection, uptake of CT LCS stays low at 18% by numerous estimates, and a chance to stop hundreds of LC deaths has been misplaced. Lately, a number of critics who had lengthy suggested towards CT LCS or for proscribing eligibility are actually advocating molecular strategies (by which they maintain a proprietary curiosity) as “pre-tests” to find out eligibility for CT scanning.
One such particular person is Peter Bach, who now serves because the chief medical officer of Delfi Diagnostics. The corporate revealed its preliminary outcomes in Nature Communications, which subsequently revealed my critique of the examine. DELFI has now revealed a second article on using their molecular “fragmentomics” as a “pre-test” for computerized tomographic lung most cancers screening (CT LCS). This potential case-control examine offers stronger proof than their earlier retrospective information, however the paper, idea, and outcomes require scrutiny.
The authors start by citing the low uptake of CT LCS as an essential purpose we want a pre-test. They use for instance the case of colon most cancers screening, the place, regardless of comparatively low sensitivity, molecular screening of each stool and blood misses important numbers of colon most cancers and has discovered broad enchantment and up to date regulatory approval.
This argument is unsound. Colonoscopy screening is disagreeable (private expertise); the preparation requires consuming a big quantity of an unpalatable liquid, punctuated by frequent pressing journeys to the bathroom. The next day is misplaced in journey to an outpatient middle, present process colonoscopy and restoration from deep intravenous sedation. Moreover, there are dangers of issues if biopsy removing of polyps is important.
In contradistinction, CT LCS screening requires no must undress and no IV, only a minute or two spent mendacity on a padded platform and some transient breath-holds. Personally, I discover this course of to be much less uncomfortable than a venipuncture.
Whereas the manuscript precisely reviews that uptake of CT LCS is low, it doesn’t focus on the function of three authors, Mazzone, Bach, and Silvestri, in contributing to the lengthy delays in screening implementation. These authors really useful towards inhabitants CT LCS or for limitation of screening for a lot of years, revealed inaccurate info suggesting that after prognosis of LC by CT LCS, just one in 5 would survive, and urged an in any other case wholesome girl athlete to “run away” from the CT scanner. In addition they suggested cessation of screening in the course of the COVID pandemic. For these authors to now specific disappointment on the present low uptake is cynical at greatest.
The interpretation of examine information is extra problematic. As famous earlier, the intent and objective of CT LCS are based upon the power of CT scans to detect lung most cancers at a really small dimension. At this level, the prospect of metastasis to lymph nodes or distant organs may be very low, and treatment is achievable. Such CT-identified lung cancers may be handled safely, with low complication charges, utilizing minimally invasive, partial lung resection or radiation remedy, even in aged sufferers with co-morbid illness. Survival following remedy stays very excessive (> 80%), extending to 10 and even twenty years. A corollary remark is that there’s little utility for a blood check that may detect massive or advanced-stage lung cancers. These cancers current with signs, after which survival, even with optimum remedy, stays poor.
Does the proof present that fragmentomics can detect early-stage LC?
The present Delfi examine reported the check’s sensitivity as 71% in stage 1 sufferers and far greater percentages in phases 3 and 4. However is a check excluding, at minimal, 29% of sufferers with lung most cancers from subsequent CT screening useful and even acceptable? If a optimistic fragmentomics check have been required earlier than an individual was eligible for CT LCS, at the very least 29% of these with lung most cancers would go undiagnosed to current later with extra superior, much less treatable, symptomatic illness.
Moreover, the 71% sensitivity estimate itself seems to be unrealistic. The supplemental information offers pertinent info. Solely 59% of 92 Stage 1 lung cancers have been categorized as Stage 1A, with an higher dimension restrict for the tumor of three cm. This suggests that 41% have been bigger, with a decrease probability of treatment. In fashionable CT LCS packages, the imply diameter of LC detected is under 1.5 cm. Cancers recognized throughout annual repeat screening are sometimes smaller than 1 cm. in diameter. Provided that we’ve got strong info displaying progressively higher long-term survival with smaller-size lesions inside stage 1A, it’s critically essential that molecular screening checks display their capability to detect equally small lung cancers.
So far, DELFI has not but supplied information to point out that their check can safely be included as a pre-test right into a diagnostic algorithm for lung most cancers screening.
To make that case, molecular diagnostic firms should concurrently check a potential cohort of CT LCS-screened sufferers to find out the sensitivity of fragmentomics or different molecular checks in sufferers with CT-screen-detected lung most cancers. Happily, such a potential cohort examine is scheduled to open in Europe within the rapid future, the place 26,000 folks in 6 European international locations shall be screened for lung most cancers with CT LCS. 9 thousand individuals will concurrently be examined utilizing the fragmentomics methodology.
This examine has the potential to reply the essential query of what share of these in danger for lung most cancers who’re eligible for insurance coverage protection could be excluded from CT LCS by a false destructive molecular display screen. Primarily based on the present examine, early Stage 1A illness detection shall be far decrease than the authors acknowledged objective of 80%, and in a pre-test algorithm, unacceptably exclude many from participation in CT LCS.
To conclude, underneath the idea that “one image is value a thousand phrases,” I invite the reader to view the picture of DELFI check outcomes, illustrating check scores in examine topics with no most cancers and with stage 1 lung most cancers.
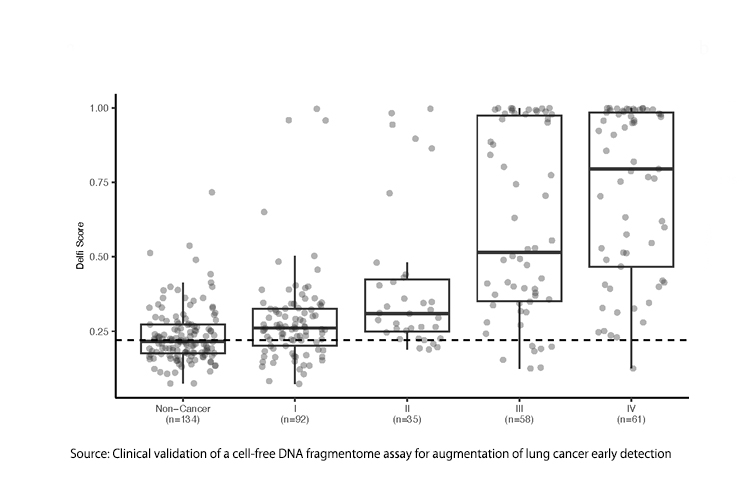
Does fragmentomics actually discriminate between these with Stage 1 lung most cancers and people with no most cancers in any respect?
CT LCS does a greater job. What’s the medical worth of a screening check for a extra definitive screening check?
{kind=link}