
Background
On this part we’re presenting the recognized difficulties met when recruiting PC (palliative care) sufferers in analysis initiatives, and the objective of this paper: investigating how these difficulties apply to PC sufferers with hematologic malignances. We used the realist (see Field 1) strategy for this, as we developed an Preliminary principle (offered at the start of the “outcomes” part) and we “refined it” by way of an proof knowledgeable course of, consisting of various steps (see “knowledge assortment and evaluation” in “supplies and strategies” part) and produced a extra refined, ultimate principle of what works, for whom and in what circumstances in enrollment of palliative care sufferers with hematological malignances (reported on the finish of the “outcomes” part).
Field 1 Glossary of phrases of realist methodology.
Realism: theory-driven analysis strategy, which produces evidence-informed theories, to higher perceive how an intervention works, for whom and underneath what circumstances, by way of the seek for underpinning mechaninsms (“retroduction”).
CMO configuration:
Context: environmental backdrop parts of an intervention or program (ig: legal guidelines, cultural norms). Context in realist principle describes “in what circumstances and why interventions or applications ‘work’”.
Mechanism: sources provided in a selected context (ig: info) and reactions of individuals concerned (ig: belief or engagement). It ought to present an “an explanatory account of how and why applications offers rise to outcomes”.
End result: results of particular mechanisms in an outlined context, each meant or unintended (ig: adherence to a therapy).
Preliminary Tough principle (IRT): speculation of underpinning mechanisms in a program or intervention, normally, within the type of “if…then” statements, that must be furtherly examined.
Refined principle: theorization ensuing from the testing of IRT by way of the evaluation of the gathered proof.
Sufferers with superior hematological malignancies undergo from a really excessive symptom burden and psychological, religious, social, and bodily signs comparable with sufferers with metastatic non-hematological malignancy (1–4).
In settlement with the brand new World Well being Group suggestion (5) the proof from research carried out in sufferers with stable tumors and hematologic sufferers’ symptom burden means that an earlier and built-in provision of specialised palliative care has the potential to enhance their high quality of life and cut back useful resource consumption by way of efficient administration of psychological and bodily signs, applicable relationships, efficient communication, and assist in decision-making. Palliative Care examine design should take into consideration intrinsic methodological challenges, such because the unpredictability of illness development, recruiting difficulties, and excessive attrition charges (6). Furthermore, final result measures that assessed the acceptance of the examine by the individuals had been incessantly absent (7) and RCT (Randomized Managed Trial) design could also be extra incessantly related with people who find themselves unwilling to be enrolled, aseven the usage of phrases like “randomization” and “placebo” (6), could be negatively perceived by the sufferers. Within the different hand,a language perceived as clear, and non-technical in that particular tradition, and the usage of phrases extra oriented to symptom administration then to palliation might have a optimistic impression.
Trials encountered enrollment challenges; for instance, the consent strategy price within the ENABLE III trial of early versus delayed initiation of concurrent palliative care was 44%, with a wide range of causes given by approached sufferers for declining participation (7, 8).
Thespecialist’s opinion concerning the experimental arm concerned within the trial proposal also can affect the enrollment (6, 9).
If they’ve the notion of “failing the affected person”, or including burden, or in the event that they lack religion within the proposed intervention, when referring to palliative care, as a result of they lack religion within the particular analysis or intervention proposed, fears to talk about prognosis, or understand the enrollment process as too demanding for the standard care employees, this may need a destructive impression on the general enrollment (10). Of their examine, White et al. state that over three quarters of interviewed sufferers said that they’d be fascinated with trial participation if their physician made it clear that he/she was eager for participation (6). The absence of signs can lower sufferers’ motivation, and on the whole sufferers have to see some related potential private acquire, because the entry to further care or a greater symptom administration (when they’re already current), or really feel that their contribution could be useful to others. Organizational elements also can have an impact, akin to if the affected person should attend a number of visits or journey additional to obtain the provided service.
Little is thought about particular analysis in PC concerning hematologic most cancers sufferers.
Research confirmed heterogeneity within the inhabitants, PC intervention, illness trajectory and therapy part (11). Solely within the final 2 years some evidences on effectiveness arose on excessive symptomatic hospitalized sufferers by EL-Jawahri et al. (12).
Following the WHO suggestion, we initially developed a PC intervention built-in with customary hematological care (13). This pilot examine was primarily targeted on assessing the feasibility of the PC intervention. Secondary goals included exploring its acceptability by sufferers, professionals and caregivers and amassing preliminary info on its effectiveness. Our examine design was mentioned with hematology colleagues to higher perceive suggest it and the inclusion standards appropriate for the feasibility trial together with sufferers at their final lively therapy (see Desk 1).
Nevertheless, the enrollment for this protocol has been troublesome; it began in November 2018 with sufferers and caregivers; we enrolled 15 sufferers in 3 years.
It’s important for our analysis crew to know the explanation for this low accrual, associated to sufferers, professionals, trial itself or group. We consider it must be attention-grabbing to match our expertise with different realities all around the world.
On this paper we described a realist synthesis (14, 15) (learn Field 1 for particulars on realist methodology), based mostly on our earlier Assessment, a fast evaluation on Hematologic most cancers affected person and analysis in Palliative Care (ultimate test March 2022) and consultants ‘opinion on PC trials for hematologic most cancers sufferers.
Ultimately, We (11) built-in these knowledge with our expertise.
Therefore, the goals of the present examine had been:
● to supply an summary of difficulties in sufferers enrollment in palliative care research, particularly in hematologic malignancies, exploring the consultants’ standpoint, literature overview, our expertise.
● to elaborate a realist synthesis of enrollment in palliative care intervention for hematologic most cancers sufferers
The outcomes of this examine could be related for growing structured intervention proposals concerning hematologic most cancers sufferers in PC trials or to provide some options to our colleagues concerned in analysis protocol on this advanced matter.
With this in thoughts, as anticipated by the realist strategy, we geared toward producing a theoretical contribution, ranging from an “Preliminary Tough Concept” (IRT) at the start of the method and ending with a extra refined model of it, because of our analysis work.
Supplies and strategies
The method that we adopted may very well be thought of a strategy of realist synthesis; we determined to incorporate secondary research in our revision, which isn’t typical, and we examined our Preliminary tough principle with an unbiased examine.
This a part of the method is suitable with the realist logic, however it’s not a hard and fast stage of normal analysis methods in realist synthesis. We thought of as our information for this manuscript the “High quality requirements for realist synthesis for researchers and peer-reviewers” (16, 17) of the Rameses mission.
In line with realist evaluation methodology, our first literature session aimed on the growth of a tough principle (IRT), that additional analysis and professional session aimed to refine the IRT, specializing in what appears to work higher, for whom, and the way, describing it by way of Context-Mechanism-End result (CMO) configurations (see Field 1 “glossary of phrases of realist methodology”).
The preliminary tough principle was based mostly on a earlier systematic revision of literature from our crew (11) and our data from our private expertise in conducting a trial on PC with hematologic sufferers (see Desk 1 “Our intervention: difficulties met, and initiatives taken in response”).
We then higher specified our focus and determined to increase our search of potential mechanisms that may have an effect on the enrollment course of to contiguous fields. Along with the seek for CMOs concerning the enrollment of hematologic sufferers into PC research, we looked for articles describing CMOs related within the referral to palliative care in hematological sufferers. (Analysis technique reported in Desk 2, the place we reported each the shift of focus of our analysis and the correspondent article choice course of, as instructed in “high quality requirements for realist synthesis”, customary 5 and 6) (17). That is an instance of “progressive focusing”, a well-established method in qualitative analysis through which the main target of the inquiry is iteratively clarified by reflection on rising knowledge (50).
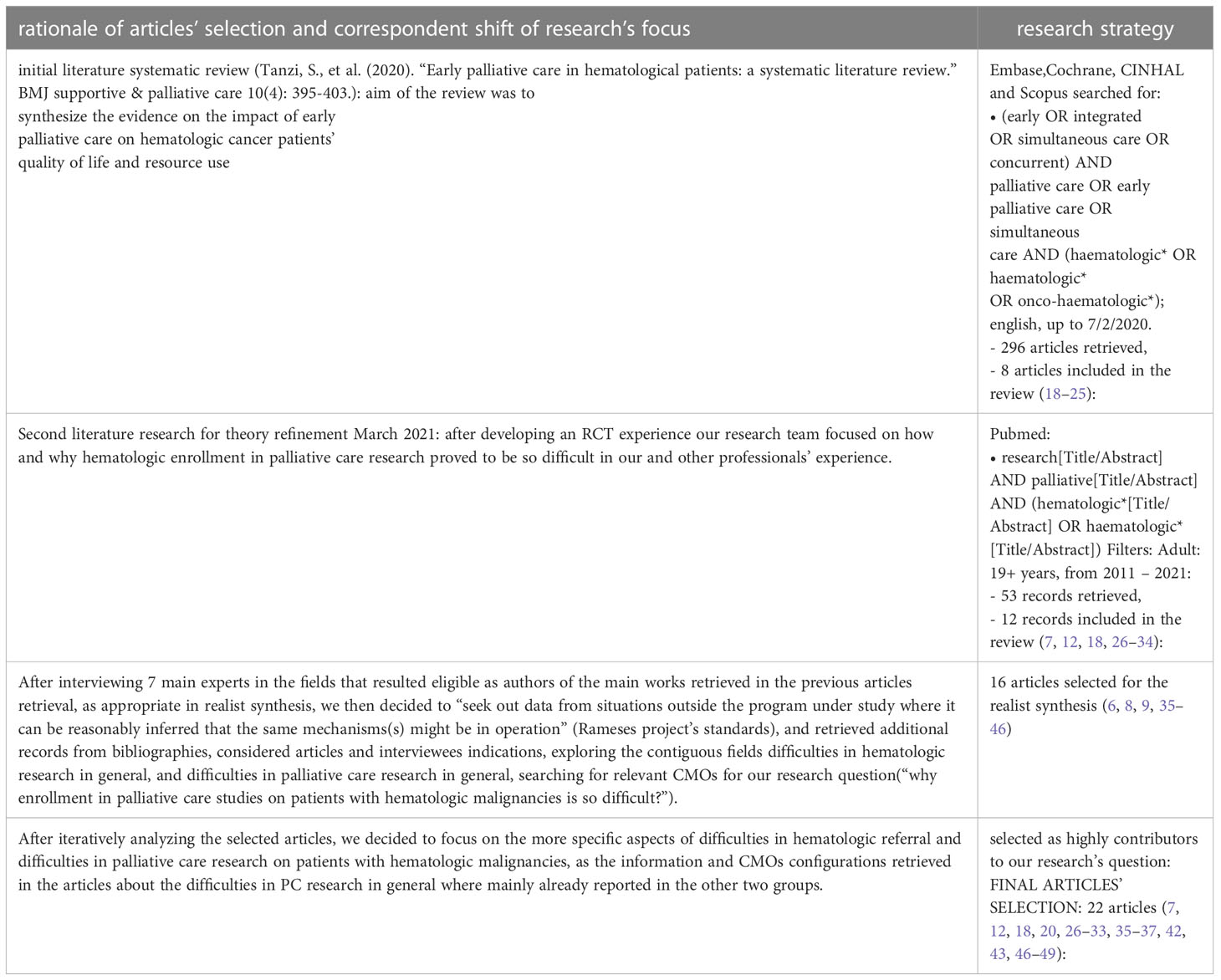
Desk 2 Articles’ choice.
We derived an interview information (see appendix 1 “the interview information”) to gather knowledge concerning the completely different analysis groups which might be conducting related research. The interview was developed following the suggestions by the RAMESES mission for “realist interviews” (17, 51).
Knowledge assortment and evaluation
Steps in growing our ultimate principle had been proven in Determine 1 “phases of analysis”.
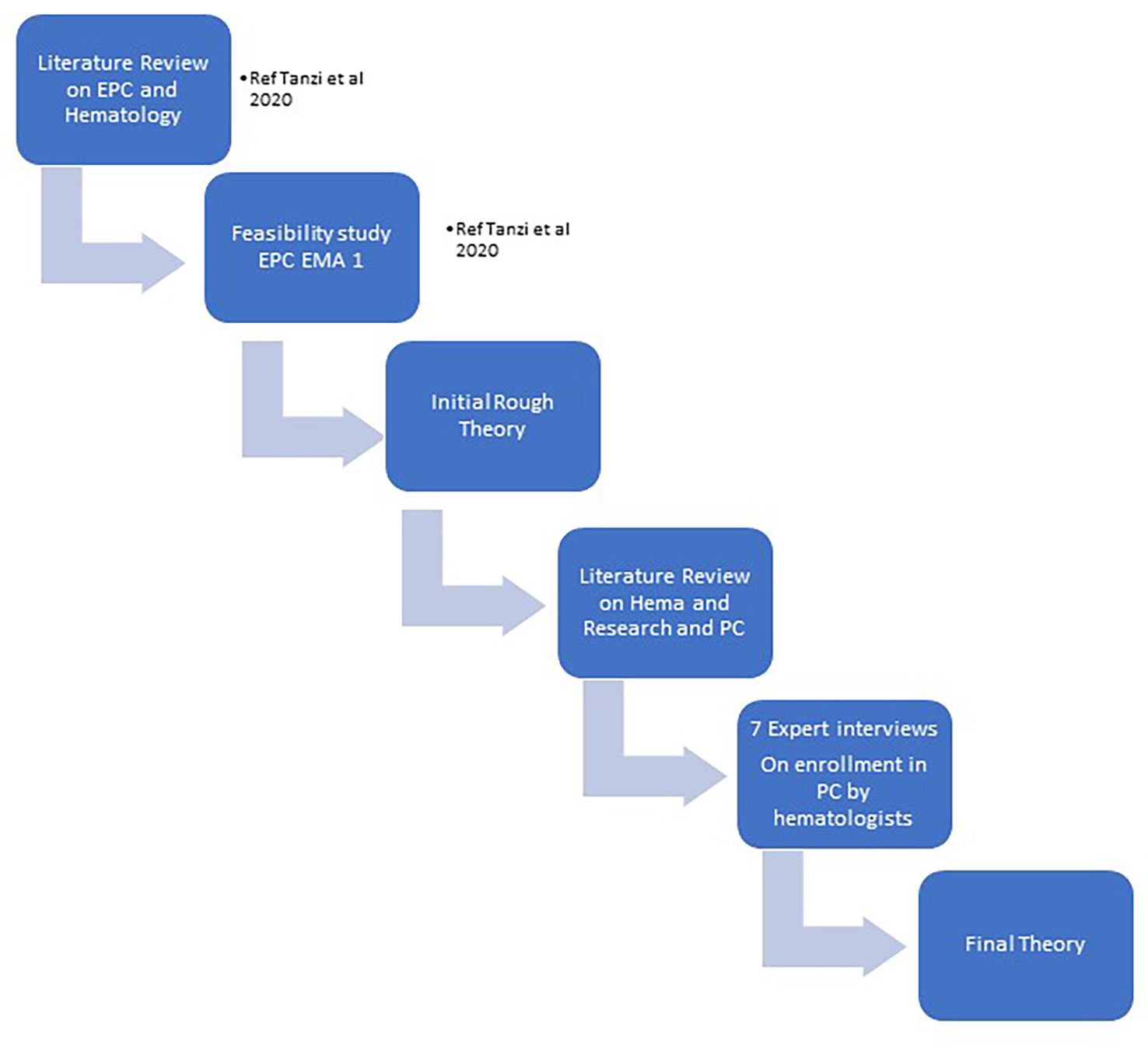
Determine 1 The phases of analysis.
They had been:
● STEP 1: we developed our IRT ranging from literature evaluation on Early Palliative Care and Hematologic most cancers sufferers and our expertise in a pilot feasibility trial
● STEP 2: we looked for related palliative care research performed with hematologic sufferers and for ongoing trials.
We analyzed the obtainable supplies (printed papers, protocols and summary), utilizing an appraisal course of through which we made a primary choice based mostly on summary’s pertinence, after which a second appraisal ranking the full-text articles based mostly on their relevance (“excessive”, “medium”, “low”, “none”). Research traits (e.g. pattern sort and measurement, sort of analysis, grade of proof) and theoretical contribution (e.g. ‘how’, ‘why, ‘in what circumstances’) had been tabulated on an Excel spreadsheet.
● STEP 3: we developed a listing of the retrieved CMOs, linking them to the completely different research, to have an operative abstract of the principle mechanism that appeared more likely to have an effect on hematologic research’ enrollments (see appendix 2).
● STEP 4: we developed an interview information based mostly on the CMOs’ record and the instructed pointers for authors’ interviews in realist evaluations; we then contacted the authors of the analysis that we analyzed to collect further info on their research and to match our findings with the consultants’ opinion (see appendix 1).
In October 2020, we despatched a primary e mail to ask the supply for an interview; in December 2020 -March 2021 we performed 7 interviews to the researchers concerned in palliative care on sufferers with hematologic malignancies interventions. GM performed audio-recorded telephone interviews with key informants of researcher groups, purposively chosen in response to the next traits: having performed a palliative care examine on hematologic most cancers sufferers printed in literature, trials ongoing (referring to trial.gov registration, final analysis July 2020) or printed analysis protocols. Two consultants had been additionally contacted based mostly on their works offered in congresses’ summary. The semi-structured interviews had been transcribed verbatim by GM. The authors of the two trials ongoing didn’t reply to our invitation.
Each authors searched the transcripts and the articles for potential context, mechanisms, advert outcomes configurations that would emerge and refine the preliminary tough principle (see Desk 3).
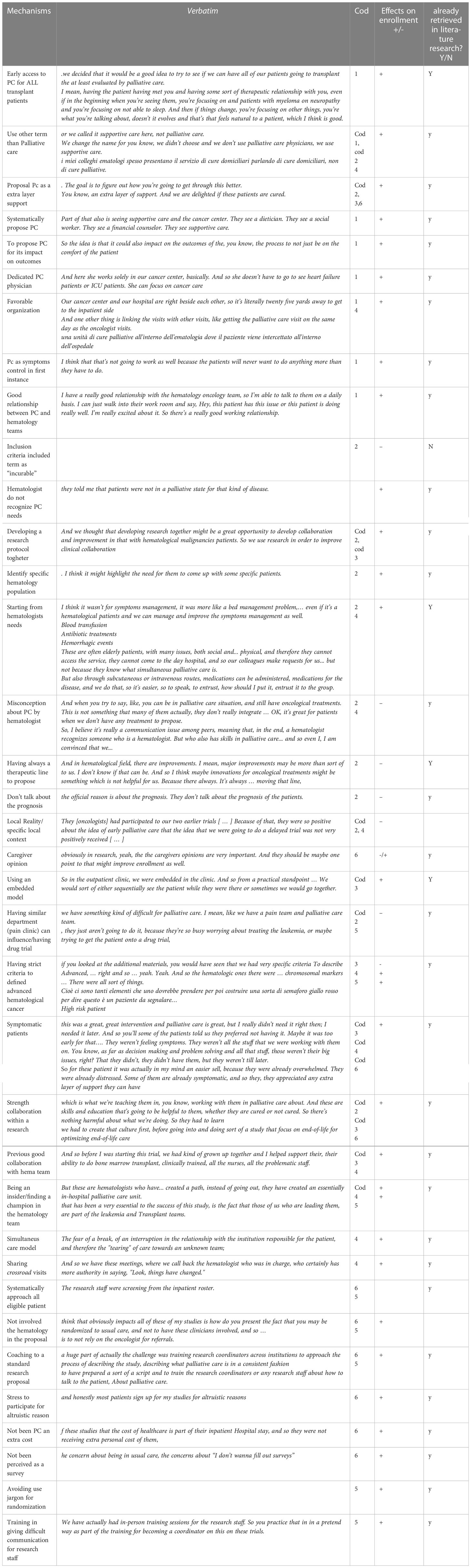
Desk 3 CMOs from the interviews.
Ethics
This Analysis mission didn’t embrace the gathering, processing, or evaluation of non-public or delicate knowledge of an occasion. Accordingly, the analysis didn’t require evaluation or approval by the Ethics Committee. However, particular participant safety procedures had been adopted: researchers requested individuals to comply with take part within the survey and interviews on a voluntary foundation by e mail, and to provide their knowledgeable consent orally through the audio registered telephone name.
Outcomes
Preliminary tough principle
We developed our IRT by way of a printed systematic evaluation (11) and the testing in our context by way of a trial (13). We tried to use some instructed enhancements through the enrolment of our analysis examine: some attentions had been deliberate simply from the start of the examine and others had been added through the enrolment course of (see Desk 1 “our intervention”).
Enrollment in palliative interventions have its difficulties, however hematology has some particular obstacles, resulting in further difficulties to enrollment and subsequent growth of latest high-quality data.
Further options that may negatively impression enrollment in PC interventions on sufferers with hematologic malignancies most likely are:
● Problem in prognostication by hematologists:
● Illness growth: uncertainty in its trajectory (additionally for the appearance of potential lifesaving therapies-as CAR T-cell) and consequently on referring to PC.
● On the opposite finish, sufferers appropriate of a PC intervention had been recognized between very “finish of life” inhabitants (life expectancy of days/few weeks)
● Defining goal inhabitants: Problem to know which hematologic inhabitants may gain advantage most from PC service, based mostly on sufferers’ wants as perceived by hematologists
● Organizational challenges: particularly for ambulatory outpatients, it’s onerous to bear in mind the opportunity of enrollment in non-pharmacological protocol by way of peculiar care. Furthermore, generally clinicians wanted to start out the allegedly final line of remedy in a very brief time, and palliative care analysis and randomization was not potential
Concept refinement course of
We refined our preliminary principle by way of a) literature analysis for related mechanisms and b) interviews to consultants within the fields.
We’re presenting our outcomes based mostly each on their supply of retrieval (“CMOs literature analysis” and “CMOs in interviews”), and as our “refined principle”, a potential world theorization of how the completely different CMOs could be theoretically associated.
CMO in literature analysis
In our literature analysis, we chosen some related mechanisms that may have an effect on the enrollment course of. We hypothesize that if hematologists don’t discuss with PC on the identical time, they don’t enroll in a palliative care trial.
So, for the goal of this mission we wrote 2 tables (see appendix 2):
CMO on patterns on referral to PC by hematologists
CMO on particular patterns on PC analysis for hematologic most cancers sufferers
Palliative care referral for hematologic most cancers sufferers
This group of CMOs focuses on the difficulties of referring to PC by hematologists and the mechanisms which have an effect on it.
A few of these M regard the mannequin of integration between hematology and PC and different organizational difficulties: strict standards to entry to hospice, for instance, lack of house and time to debate about PC, hospital tradition targeted on curing, being in numerous division and never having entry 24/24 hours to PC service, might cut back referral to PC. A linear (from starting to finish) mannequin greater than a sequential one (PC solely when hematologic care is concluded) might enhance PC referral as having clear management on sufferers between the two staffs. Poor communication between staffs is detrimental even for PC referral.
Relation between hematologist and laptop professionals with reciprocal acknowledgment might enhance PC referral, not seeing referring to PC as a failure or a deskilling. Perceived self-efficacy by hematologists and misconceptions about palliative care might cut back referral to PC service. The time period PC itself may very well be prevented. Affected person’s situations as asymptomatic sufferers or sufferers with unrealistic expectations might cut back the combination between the two staffs. Hematologic sufferers might have particular wants not addressed by PC and sudden illness trajectory makes troublesome to acknowledge PC wants. Hematologists difficulties to suggest a guide inside a long-time relationship with affected person, late finish of life discussions and unrealistic expectations from lively remedies might cut back PC referral by hematologists.
Palliative care analysis for hematologic most cancers sufferers
On this group we analyzed mechanisms instructed from the scarce literature on enrolment in PC for hematologic most cancers sufferers (7, 18, 35–37). The mechanisms underlying the low enrollment appear to be fairly much like the well-known mechanisms in PC on the whole (8, 9, 38–42, 52, 53), with some extra specificity concerning this subgroup as the issue to outline a transparent prognosis. Figuring out sufferers with highest supportive wants might enhance feasibility and acceptability of future main palliative care in hematologic malignancy trials. Furthermore, lack of affected person curiosity within the matter of palliative care analysis additionally probably affected the feasibility.
CMOs in interviews
The interviews with professional partially agreed with the outcomes from the literature, however in addition they contributed so as to add some vital perception into our analysis query (see Desk 3 “interviews’ mechanisms” and Desk 4 “interviewers traits”). Consultants’ interviews instructed that the preliminary recognized inhabitants must be wealthy in signs burden to start out constructing a collaboration with hematologists.
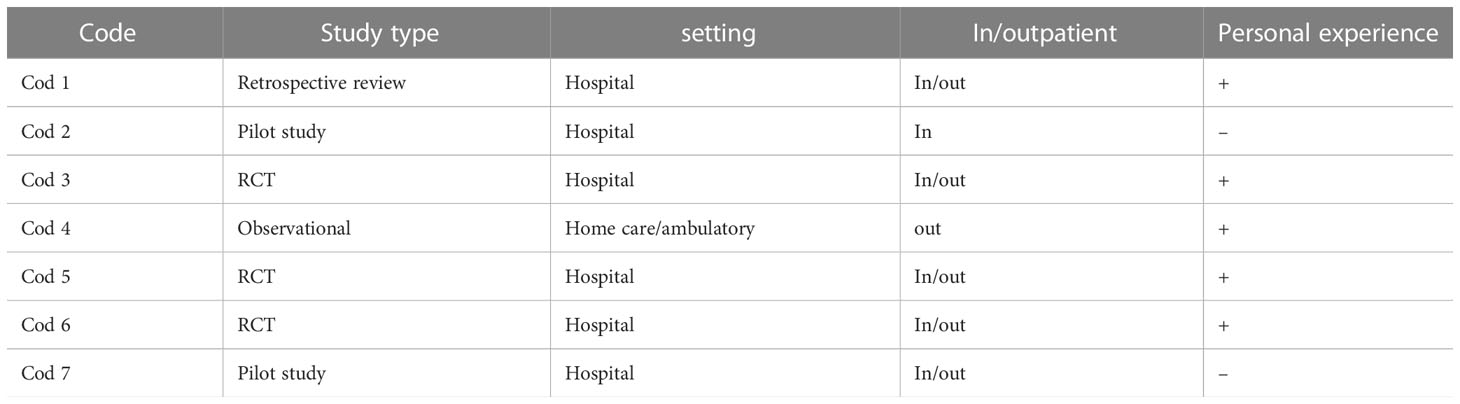
Desk 4 Interviewee traits.
Consequently, in a second time, end-of-life sufferers may very well be co-managed between the 2 staffs, with a simultaneous strategy. Furthermore, being a part of the hematologic crew or being perceived like an insider appear to be the profitable factor within the RCTs realized till now.
Lastly, trials with inpatients -as transplanted sufferers, for instance – may very well be simpler to conduct, as a result of excessive signs burden and the entry facility to the ward.
Alternatively, failure expertise collected from the interviewed consultants are described as linked to the inhabitants goal definition as “incurable”, a criterion onerous to acknowledge for hematologists.
Furthermore, the hematologist standpoint on Palliative Care is crucial for each discuss with PC and suggest a PC trial.
Refined principle
An vital discovering of this evaluation was that ‘success options’ didn’t appear to be intrinsic to any particular single examine design or sort of analysis, however the results of many alternative interactions between completely different contexts and mechanisms. “Social change principle” by Homans was utilized by Salins to elucidate the potential issues in referral in palliative care (47), together with hematology. We chosen this principle as versatile and helpful sufficient for use to elucidate the issues in enrollment in PC research in hematologic sufferers too. In line with this interpretation, referral is a social interplay, and relies on the notion of social actors of this interplay as able to offering a type of reward and keep away from a price. As represented in Determine 2, it’s believable that each actor concerned can create attrition within the enrollment course of. However as said each within the reviewed literature and within the consultants ‘opinions, it’s potential to design a examine or a scientific setting to create a notion of a extra favorable reward/prices relation for all of the actors concerned: this could be seen because the “intermediate mechanism”, on which completely different type of interventions would possibly have an effect.
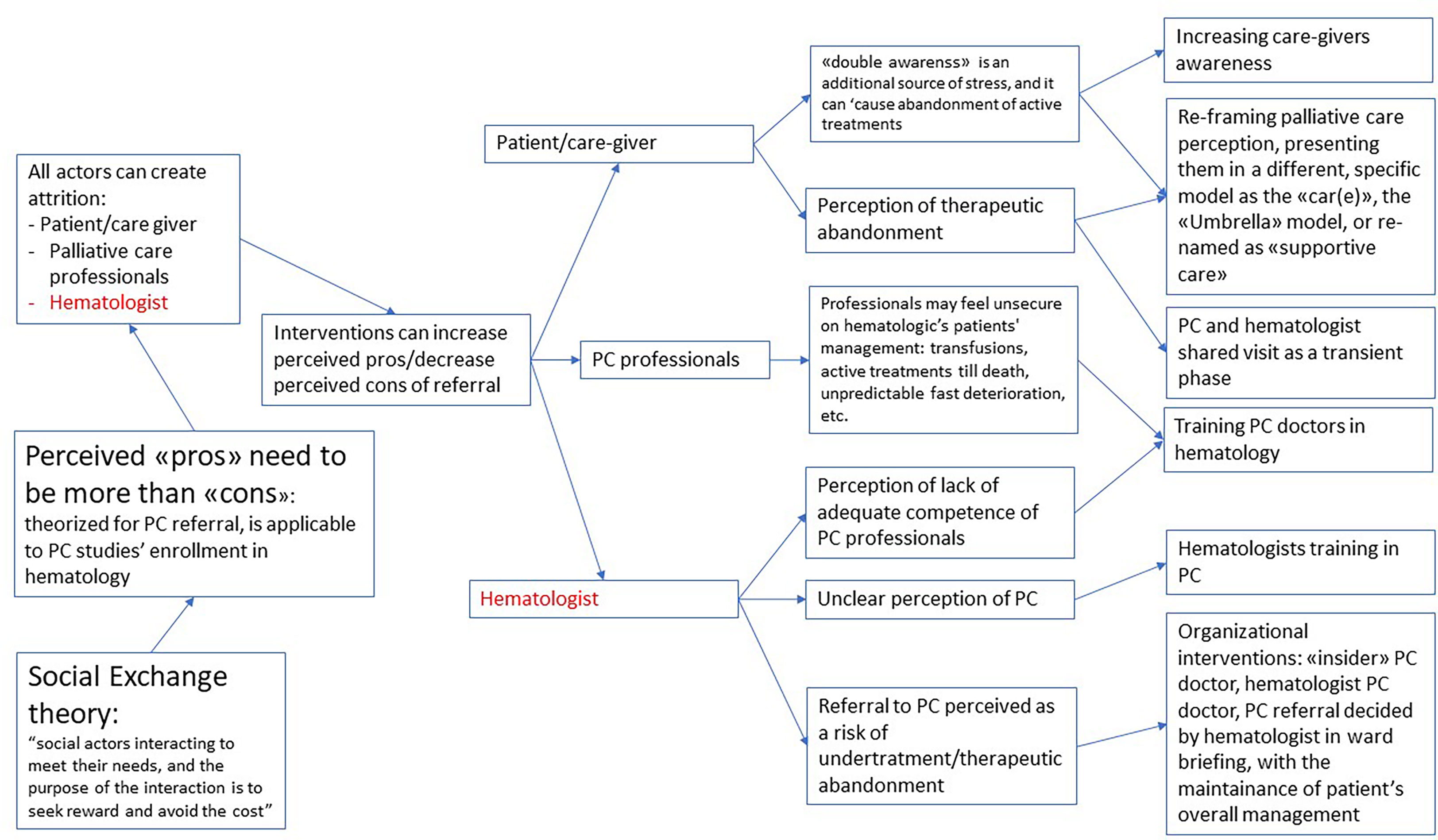
Determine 2 Refined principle: what works, for whom and through which circumstaces, when enrolling hematologic most cancers sufferers in palliative care?
It’s potential to intervene on the notion of sufferers and caregivers, the place the “double consciousness” (26) of probably deadly growth of the illness and on the identical time probably life-prolonging intervention creates a excessive stress. For example, reframing their notion of palliative care by way of the usage of a distinct time period (as “supportive care”) (27) or the reason of a distinct framework for palliative take care of sufferers with hematologic malignancies because the “CAR(E)” or “Umbrella” mannequin (43), and even with an specific resolution to create a better involvement of the care giver in partial substitution of the affected person.
It’s additionally potential to extend the self-efficacy of palliative care docs, by way of particular hematologic coaching, contemplating the particular variations of this sufferers’ inhabitants.
Nevertheless it’s extremely probably that the extra related actor within the course of could be the hematologist. Many potential interventions would possibly result in a greater notion of the benefits of PC referral.
An unclear notion of referral as a potential supply of undertreatment could be addressed with organizational changes, as having a PC hematologist, or a palliative care session that’s mentioned within the ward assembly and retains the affected person underneath the hematologic administration.
As a consequence, (see Determine 3) the notion of the completely different actors could be the important thing factor to result in an intervention modulated on the traits of the particular setting through which the examine could be developed, specifically the notion of hematologists. A stronger, already present relationship between the 2 groups would possibly suggest the prospect of engaged on extremely advanced wants. On the opposite finish, a brand new relationship would possibly require a neater process to start out, as addressing extremely symptomatic sufferers (ig, sufferers present process transplantation).
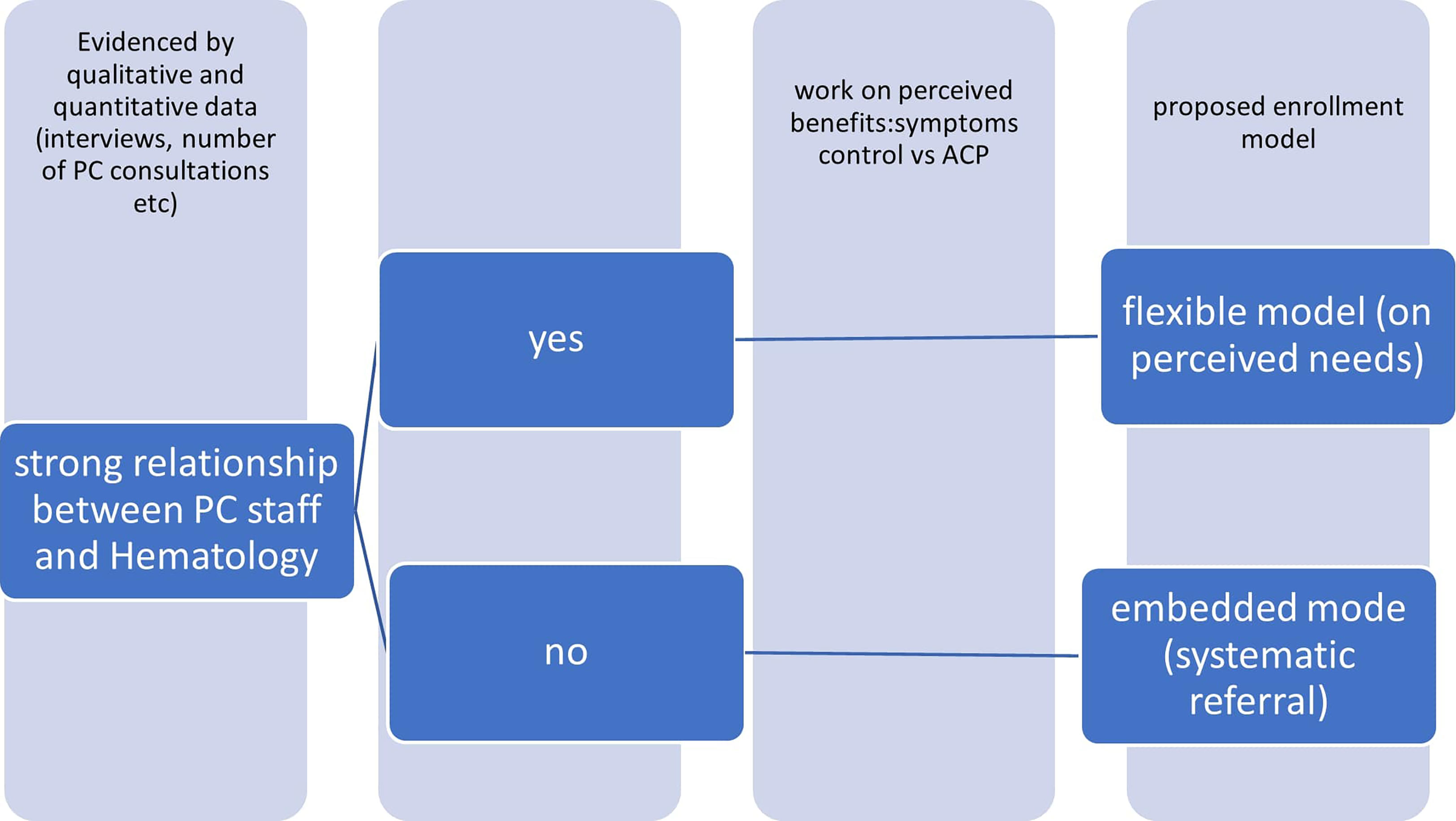
Determine 3 Groups’ relationship and enrollment.
Dialogue
This synthesis from literature and consultants ‘opinions permits us to deepen the subject of enrolment in PC trial in hematologic most cancers sufferers.
As highlighted by our outcomes, the issue of enrolling hematological sufferers in palliative care trials overlaps with dynamics inherent within the referral to PC companies by hematologists, on the whole.
We outlined our normal refined principle as a “ecological principle of enrollment in palliative care analysis on sufferers with hematologic malignancies”.
As a refinement to our preliminary record of CMOs impacting the enrollment course of, we chosen the “social change principle” (SET) of Salins (47) as a related mannequin for our theoretical building. In his SET, he theorizes that oncologists have to have a transparent notion of the benefits that they may get from the referral to palliative care, and that these benefits have to outbalance the prices.
This mannequin is helpful to elucidate the issue of enrollment in palliative care intervention in hematologic sufferers too and may very well be built-in with different theoretical features particular for this area. We face in hematologic sufferers the particular issue of “double consciousness” (as theorized by Gerlach (26)) that places the sufferers and the caregivers on a selected rigidity as a result of double chance of getting a fast deterioration of well being situations to loss of life or attending to a disease-free time period because of the medicines. Making use of the SET mannequin to hematology intervention, we’d see how this facet of “double consciousness” must be managed each by well being professionals and sufferers and caregivers. Well being professionals will then be assessing their professionals and cons of referral, figuring out that the prices of the referral would possibly end in much less consciousness of curing potentialities and fewer give attention to obtainable remedies.
One other related CMO that we added to our preliminary principle, is that palliative care wants the PC professionals to be actually versatile, to extend referral to PC of sufferers with hematologic malignancies, trying to find probably the most appropriate mannequin for his or her setting. Whereas we listed a number of features that would have an effect and must be addressed whereas designing the intervention, if we begin from the SET principle, it appears protected to theorize that each intervention ought to begin from the evaluation of the notion of the hematologists of the potential benefits and drawbacks of the referral to palliative care. A primary distinction must be between interventions which might be constructed on a robust relationship between PC employees and hematologists, and interventions which might be developed independently from an already relationship between the groups. Typically, these interventions would possibly implicitly be designed to construct a greater relationship by the leaders of this system.
Quantitative parts may very well be informative on the extent of integration; whereas qualitative knowledge might assist deciding on the weather that may very well be addressed by an intervention geared toward reaching a extra cooperative setting.
The profitable experiences reported of enrollment of hematologic sufferers in palliative care had been all based mostly on a earlier optimistic expertise of cooperation between the 2 groups (7, 18). It could be unlikely that the enrollment course of may very well be profitable in a context the place the intervention itself goals at acquiring a greater interplay between the 2 groups.
Some interventions are potential and appear extra more likely to work, and all of them could be interpreted as an effort to extend the professionals/cons ratio and the notion of the palliative care contribution within the hematologists.
Mere technical enhancements (akin to a remembering e mail or a telephone name from the researcher) in addition to merely hypothesizing a distinct examine design (42) appear to not be capable to clear up the query and would possibly result in miss the extra related factors.
The contamination of information with a Palliative care/hematology mannequin that’s not solely built-in however embedded (44) would reply each to organizational issues and to these associated to misconceptions on PC; each professional interviews and knowledge from literature verify this suggestion.
The well being care professionals gate keeping-where the professionals don’t acknowledge PC needs- was acknowledged as a barrier to PC enrolment by the literature (42) and appears to be logically relevant within the hematologic setting too. An integrative mannequin “fluctuant, versatile and based mostly on sufferers’ wants”, the place these wants are detected by hematologists has been instructed as a potential mannequin of optimum integration (3). Nevertheless it could be helpful to contemplate the opportunity of an much more embedded mannequin, the place PC is nearly “compelled” in hematology ward’s every day work. It might reduce the burden of the intervention each for sufferers and scientific employees and overcome the difficulties by hematologist to acknowledge PC wants particularly in asymptomatic sufferers. Furthermore, having a PC doctor/nurse as a member of the hematologic crew might result in understand palliative care as a routine element of the affected person care.
In line with this, an extra mechanism that could be helpful when it comes to integration is the coaching of hematological professionals in palliative care and in understanding deeply the palliative care strategy, whereas coaching palliative care practitioners as nicely to the specificities of the hematological affected person, as instructed by many authors (26, 28–30, 45).
Our consultants’ interviews additionally instructed that enrolling solely symptomatic sufferers may very well be a extra preliminary intervention; nonetheless, an early strategy additionally for asymptomatic sufferers might change the tradition/enhance the acceptance between palliative care professionals and hematologist. The referral not just for bodily wants but in addition social, psychological, moral and religious ones, must be learnt and improved (26, 46).
Unpredictable course of hematologic malignancies might negatively impression the enrollment.
Utilizing goal and systematic standards for enrollment (as conducing a primary evaluation on the record of transplants, or having an automated flagging and reporting of sufferers with unhealthy prognosis standards) would keep away from this lack. Synthetic intelligence has had a rising enchancment for this sort of issues (54).
Limitations
The general high quality of a evaluation is strongly influenced by the standard of the first research thought of. The issue in gathering firsthand knowledge on palliative care sufferers is the very purpose why this strategy could be attention-grabbing, as we tried to supply a theoretical contribution based mostly on what is thought, what’s guessable and what’s not recognized to assist navigate this troublesome area.
A realist evaluation is an evidence-informed evaluation, who is simply partially proof based mostly, as a part of the trouble on this particular sort of evaluation is attempting to supply a theoretical contribution from the obtainable knowledge. We tried to counsel potential options and helpful hyperlinks between what’s perceived as related on this area, attempting to start out from making specific what’s “apparent” for the researchers within the area however not so apparent for the readers.
This strategy limits the precise generalizability of our options, however encourages researchers to attempt to verify or problem our speculation, as anticipated by realist methodologies.
Conclusions
The referral to PC- because the enrollment in a PC trial – must be tailor-made on sufferers’ wants and recognizing these palliative care wants will not be easy for Hematologists.
To acknowledge the connection between PC employees and Hematology is obligatory to suggest the precise strategy, an integration versatile mannequin or on an embedded mannequin.
Consequently, we propose that anticipated outcomes must be completely different, based mostly on a preliminary analysis of the context of the intervention: whereas an intervention based mostly on a brand new relationship may need as a beginning stage the goal to handle advanced signs management, and may additionally explicitly be a part of a wider intervention that may end in constructing stronger relationships between the completely different stakeholders. On the opposite aspect, when a robust, earlier relationship between the staffs is already current, it’d enhance the prospect to handle extra advanced matters as advance care planning.
Knowledge availability assertion
The unique contributions offered within the examine are included within the article/Supplementary Materials. Additional inquiries could be directed to the corresponding creator.
Ethics assertion
Moral evaluation and approval was not required for the examine on human individuals in accordance with the native laws and institutional necessities.
Writer contributions
Each authors contributed to all elements of the manuscripts. Particularly, ST labored extra on background and dialogue and GM labored extra on “strategies” and outcomes. All authors contributed to the article and accepted the submitted model.
Funding
This work was partially supported by the Italian Ministry of Well being – Ricerca Corrente Annual Program 2024.
Battle of curiosity
The authors declare that the analysis was performed within the absence of any industrial or monetary relationships that may very well be construed as a possible battle of curiosity.
Writer’s be aware
All claims expressed on this article are solely these of the authors and don’t essentially characterize these of their affiliated organizations, or these of the writer, the editors and the reviewers. Any product that could be evaluated on this article, or declare that could be made by its producer, will not be assured or endorsed by the writer.
Supplementary materials
The Supplementary Materials for this text could be discovered on-line at: https://www.frontiersin.org/articles/10.3389/fonc.2023.991791/full#supplementary-material
References
2. Odejide OO, Cronin AM, Condron NB, Fletcher SA, Earle CC, Tulsky JA, et al. Limitations to high quality end-of-Life take care of sufferers with blood cancers. J Clin Oncol Off J Am Soc Clin Oncol (2016) 34(26):3126–32. doi: 10.1200/JCO.2016.67.8177
4. Zimmermann C, Mathews J. Palliative care is the umbrella, not the rain–a metaphor to information conversations in superior most cancers. JAMA Oncol (2022) 8(5):681. doi: 10.1001/jamaoncol.2021.8210
PubMed Summary | CrossRef Full Textual content | Google Scholar
5. Sepúlveda C, Marlin A, Yoshida T, Ullrich A. Palliative care: the world well being group’s world perspective. J Ache Symptom Handle (2002) 24(2):91–6. doi: 10.1016/S0885-3924(02)00440-2
PubMed Summary | CrossRef Full Textual content | Google Scholar
6. White C, Hardy J. What do palliative care sufferers and their kin take into consideration analysis in palliative care?–a scientific evaluation. Assist Care Most cancers (2010) 18(8):905–11. doi: 10.1007/s00520-009-0724-1
PubMed Summary | CrossRef Full Textual content | Google Scholar
7. Bakitas MA, Tosteson TD, Li Z, Lyons KD, Hull JG, Li Z, et al. Early versus delayed initiation of concurrent palliative oncology care: Affected person outcomes within the ENABLE III randomized managed trial. J Clin Oncol Off J Am Soc Clin Oncol (2015) 33(13):1438–45. doi: 10.1200/JCO.2014.58.6362
8. Schenker Y, Bahary N, Claxton R, Childers J, Chu E, Kavalieratos D, et al. A pilot trial of early specialty palliative take care of sufferers with superior pancreatic most cancers: Challenges encountered and classes realized. J Palliat Med (2018) 21(1):28–36. doi: 10.1089/jpm.2017.0113
PubMed Summary | CrossRef Full Textual content | Google Scholar
9. Bloomer MJ, Hutchinson AM, Brooks L, Botti M. Dying individuals’ views on, or experiences of, collaborating in analysis: An integrative evaluation. Palliat Med (2018) 32(4):851–60. doi: 10.1177/0269216317744503
PubMed Summary | CrossRef Full Textual content | Google Scholar
10. Firn J, Preston N, Walshe C. What are the views of hospital-based generalist palliative care professionals on what facilitates or hinders collaboration with in-patient specialist palliative care groups? a systematically constructed narrative synthesis. Palliat Med (2016) 30(3):240–56. doi: 10.1177/0269216315615483
PubMed Summary | CrossRef Full Textual content | Google Scholar
11. Tanzi S, Venturelli F, Luminari S, Merlo FD, Braglia L, Bassi C, et al. Early palliative care in haematological sufferers: a scientific literature evaluation. BMJ Assist Palliat Care (2020) 10(4):395–403. doi: 10.1136/bmjspcare-2020-002386
PubMed Summary | CrossRef Full Textual content | Google Scholar
12. El-Jawahri A, Nelson AM, Grey TF, Lee SJ, LeBlanc TW. Palliative and end-of-Life take care of sufferers with hematologic malignancies. J Clin Oncol (2020) 38(9):944–53. doi: 10.1200/JCO.18.02386
PubMed Summary | CrossRef Full Textual content | Google Scholar
13. Tanzi S, Luminari S, Cavuto S, Turola E, Ghirotto L, Costantini M. Early palliative care versus customary care in haematologic most cancers sufferers at their final lively therapy: examine protocol of a feasibility trial. BMC Palliat Care (2020) 19(1):53. doi: 10.1186/s12904-020-00561-w
PubMed Summary | CrossRef Full Textual content | Google Scholar
14. Wong G, Greenhalgh T, Westhorp G, Pawson R. Realist strategies in medical schooling analysis: what are they and what can they contribute? Med Educ (2012) 46(1):89–96. doi: 10.1111/j.1365-2923.2011.04045.x
PubMed Summary | CrossRef Full Textual content | Google Scholar
16. Wong G, Westhorp G, Manzano A, Greenhalgh J, Jagosh J, Greenhalgh T. RAMESES II reporting requirements for realist evaluations. BMC Med (2016) 14(1):96. doi: 10.1186/s12916-016-0643-1
PubMed Summary | CrossRef Full Textual content | Google Scholar
18. El-Jawahri A, LeBlanc T, VanDusen H, Traeger L, Greer JA, Pirl WF, et al. Impact of inpatient palliative care on high quality of life 2 weeks after hematopoietic stem cell transplantation: A randomized scientific trial. JAMA (2016) 316(20):2094–103. doi: 10.1001/jama.2016.16786
PubMed Summary | CrossRef Full Textual content | Google Scholar
19. Cheung MC, Croxford R, Earle CC, Singh S. Days spent at residence within the final 6 months of life: a top quality indicator of finish of life care in sufferers with hematologic malignancies. Leuk Lymphoma (2020) 61(1):146–55. doi: 10.1080/10428194.2019.1654095
PubMed Summary | CrossRef Full Textual content | Google Scholar
20. Rodin G, Malfitano C, Rydall A, Schimmer A, Marmar CM, Mah Okay, et al. Emotion and symptom-focused engagement (EASE): a randomized part II trial of an built-in psychological and palliative care intervention for sufferers with acute leukemia. Assist Care Most cancers Off J Multinatl Assoc Assist Care Most cancers (2020) 28(1):163–76. doi: 10.1007/s00520-019-04723-2
21. Loggers ET, LeBlanc TW, El-Jawahri A, Fihn J, Bumpus M, David J, et al. Pretransplantation supportive and palliative care session for high-risk hematopoietic cell transplantation sufferers. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transpl (2016) 22(7):1299–305. doi: 10.1016/j.bbmt.2016.03.006
22. Porta-Gross sales J, Guerrero-Torrelles M, Moreno-Alonso D, Sarrà-Escarré J, Clapés-Puig V, Trelis-Navarro J, et al. Is early palliative care possible in sufferers with a number of myeloma? J Ache Symptom Handle (2017) 54(5):692–700. doi: 10.1016/j.jpainsymman.2017.04.012
PubMed Summary | CrossRef Full Textual content | Google Scholar
23. Selvaggi KJ, Vick JB, Jessell SA, Lister J, Abrahm JL, Bernacki R. Bridging the hole: a palliative care session service in a hematological malignancy-bone marrow transplant unit. J Group Assist Oncol (2014) 12(2):50–5. doi: 10.12788/jcso.0015
PubMed Summary | CrossRef Full Textual content | Google Scholar
24. Cartoni C, Brunetti GA, D’Elia GM, Breccia M, Niscola P, Marini MG, et al. Price evaluation of a domiciliary program of supportive and palliative take care of sufferers with hematologic malignancies. Haematologica (2007) 92(5):666–73. doi: 10.3324/haematol.10324
PubMed Summary | CrossRef Full Textual content | Google Scholar
25. Hung YS, Wu JH, Chang H, Wang PN, Kao CY, Wang HM, et al. Traits of sufferers with hematologic malignancies who acquired palliative care session companies in a medical middle. Am J Hosp Palliat Care (2013) 30(8):773–80. doi: 10.1177/1049909112471423
PubMed Summary | CrossRef Full Textual content | Google Scholar
26. Gerlach C, Alt-Epping B, Oechsle Okay. Particular challenges in end-of-life take care of sufferers with hematological malignancies. Curr Opin Assist Palliat Care (2019) 13(4):369–79. doi: 10.1097/SPC.0000000000000470
PubMed Summary | CrossRef Full Textual content | Google Scholar
27. Booker R, Dunn S, Earp MA, Sinnarajah A, Biondo PD, Simon JE. Views of hematology oncology clinicians about integrating palliative care in oncology. Curr Oncol (2020) 27(6):313–20. doi: 10.3747/co.27.6305
PubMed Summary | CrossRef Full Textual content | Google Scholar
28. Dowling M, Fahy P, Houghton C, Smalle M. A qualitative proof synthesis of healthcare professionals’ experiences and views of palliative take care of sufferers with a haematological malignancy. Eur J Most cancers Care (Engl) (2020) 29(6):1-25. doi: 10.1111/ecc.13316
30. McCaughan D, Roman E, Smith AG, Garry AC, Johnson MJ, Patmore RD, et al. Palliative care specialists’ perceptions regarding referral of haematology sufferers to their companies: findings from a qualitative examine. BMC Palliat Care (2018) 17(1):33. doi: 10.1186/s12904-018-0289-1
PubMed Summary | CrossRef Full Textual content | Google Scholar
31. Bennardi M, Diviani N, Gamondi C, Stüssi G, Saletti P, Cinesi I, et al. Palliative care utilization in oncology and hemato-oncology: a scientific evaluation of cognitive limitations and facilitators from the attitude of healthcare professionals, grownup sufferers, and their households. BMC Palliat Care (2020) 19(1):47. doi: 10.1186/s12904-020-00556-7
PubMed Summary | CrossRef Full Textual content | Google Scholar
32. Barbaret C, Berthiller J, Schott Pethelaz AM, Michallet M, Salles G, Sanchez S, et al. Analysis protocol on early palliative care in sufferers with acute leukaemia after one relapse. BMJ Assist Palliat Care (2017) 7(4):480–4. doi: 10.1136/bmjspcare-2016-001173
PubMed Summary | CrossRef Full Textual content | Google Scholar
33. Morikawa M, Shirai Y, Ochiai R, Miyagawa Okay. Limitations to the collaboration between hematologists and palliative care groups on relapse or refractory leukemia and malignant lymphoma sufferers’ care: A qualitative examine. Am J Hosp Palliat Med (2016) 33(10):977–84. doi: 10.1177/1049909115611081
34. Scarfò L, Karamanidou C, Doubek M, Garani-Papadatos T, Didi J, Pontikoglou C, et al. MyPal ADULT examine protocol: a randomised scientific trial of the MyPal ePRO-based early palliative care system in grownup sufferers with haematological malignancies. BMJ Open (2021) 11(11):e050256. doi: 10.1136/bmjopen-2021-050256
PubMed Summary | CrossRef Full Textual content | Google Scholar
35. Bakitas M, Lyons KD, Hegel MT, Ahles T. Oncologists’ views on concurrent palliative care in a nationwide most cancers institute-designated complete most cancers middle. Palliat Assist Care (2013) 11(5):415–23. doi: 10.1017/S1478951512000673
PubMed Summary | CrossRef Full Textual content | Google Scholar
36. Maloney C, Lyons KD, Li Z, Hegel M, Ahles TA, Bakitas M. Affected person views on participation within the ENABLE II randomized managed trial of a concurrent oncology palliative care intervention: Advantages and burdens. Palliat Med (2013) 27(4):375–83. doi: 10.1177/0269216312445188
PubMed Summary | CrossRef Full Textual content | Google Scholar
37. Resick JM, Sefcik C, Arnold RM, LeBlanc TW, Bakitas M, Rosenzweig MQ, et al. Main palliative take care of sufferers with superior hematologic malignancies: A pilot trial of the SHARE intervention. J Palliat Med (2021) 24(6):820–9. doi: 10.1089/jpm.2020.0407
38. Jones TA, Olds TS, Currow DC, Williams MT. Feasibility and pilot research in palliative care analysis: A scientific evaluation. J Ache Symptom Handle (2017) 54(1):139–151.e4. doi: 10.1016/j.jpainsymman.2017.02.015
PubMed Summary | CrossRef Full Textual content | Google Scholar
39. Audrey S. Qualitative analysis in evidence-based medication: Bettering decision-making and participation in randomized managed trials of most cancers remedies. Palliat Med (2011) 25(8):758–65. doi: 10.1177/0269216311419548
PubMed Summary | CrossRef Full Textual content | Google Scholar
40. Houghton C, Dowling M, Meskell P, Hunter A, Gardner H, Conway A, et al. Elements that impression on recruitment to randomised trials in well being care: a qualitative proof synthesis. In: Cochrane database syst rev. (New Jersey, U.S.: John Wiley & Sons, Ltd Hoboken) (2020)2020. doi: 10.1002/14651858.MR000045.pub2
41. Walsh E, Sheridan A. Elements affecting affected person participation in scientific trials in Eire: A story evaluation. Contemp Clin Trials Commun (2016) 3:23–31. doi: 10.1016/j.conctc.2016.01.002
PubMed Summary | CrossRef Full Textual content | Google Scholar
42. Dunleavy L, Walshe C, Oriani A, Preston N. Utilizing the “Social advertising and marketing combine framework” to discover recruitment limitations and facilitators in palliative care randomised managed trials? a story synthesis evaluation. Palliat Med (2018) 32(5):990–1009. doi: 10.1177/0269216318757623
PubMed Summary | CrossRef Full Textual content | Google Scholar
43. Button E, Bolton M, Chan RJ, Chambers S, Butler J, Yates P. A palliative care mannequin and conceptual strategy suited to scientific malignant haematology. Palliat Med (2019) 33(5):483–5. doi: 10.1177/0269216318824489
PubMed Summary | CrossRef Full Textual content | Google Scholar
44. Ofran Y, Bar-Sela G, Toledano M, Kushnir I, Moalem B, Gil W, et al. Palliative care service integrated in a hematology division: a working mannequin fostering modifications in scientific follow. Leuk Lymphoma (2019) 60(8):2079–81. doi: 10.1080/10428194.2018.1564826
PubMed Summary | CrossRef Full Textual content | Google Scholar
45. Santivasi W, Wu Okay, Litzow M, LeBlanc T, Strand J. Palliative care doctor consolation (and discomfort) with discussing prognosis in hematologic ailments: Outcomes of a nationwide survey (SA528B). J Ache Symptom Handle (2019) 57(2):454. doi: 10.1016/j.jpainsymman.2018.12.205
47. Salins N, Ghoshal A, Hughes S, Preston N. How views of oncologists and haematologists impacts palliative care referral: a scientific evaluation. BMC Palliat Care (2020) 19(1):175. doi: 10.1186/s12904-020-00671-5
PubMed Summary | CrossRef Full Textual content | Google Scholar
48. Santivasi WL, Childs DS, Wu KL, Partain DK, Litzow MR, LeBlanc TW, et al. Perceptions of hematology amongst palliative care physicians: Outcomes of a nationwide survey. J Ache Symptom Handle (2021) 62(5):949–59. doi: 10.1016/j.jpainsymman.2021.04.021
PubMed Summary | CrossRef Full Textual content | Google Scholar
49. Payne SA, Moore DC, Stamatopoulos Okay. MyPal: Designing and evaluating digital patient-reported final result methods for most cancers palliative care in Europe. J Palliat Med (2021) 24(7):962–4. doi: 10.1089/jpm.2021.0120
PubMed Summary | CrossRef Full Textual content | Google Scholar
52. Boland J, Currow DC, Wilcock A, Tieman J, Hussain JA, Pitsillides C, et al. A scientific evaluation of methods used to extend recruitment of individuals with most cancers or organ failure into scientific trials: Implications for palliative care analysis. J Ache Symptom Handle (2015) 49(4):762–772.e5. doi: 10.1016/j.jpainsymman.2014.09.018
PubMed Summary | CrossRef Full Textual content | Google Scholar
53. Vlckova Okay, Polakova Okay, Tuckova A, Houska A, Loucka M. Views of sufferers with superior illness and their kin on participation in palliative care analysis. BMC Palliat Care (2021) 20(1):80. doi: 10.1186/s12904-021-00779-2
PubMed Summary | CrossRef Full Textual content | Google Scholar
{kind=link}