
Introduction
The first goal of treating continual section continual myeloid leukemia (CML-CP) is to stop development to extra aggressive accelerated or blast section CML, whatever the tyrosine kinase inhibitor (TKI) line, enabling sufferers to attain a life expectancy just like the final inhabitants (1). Because the approval of the primary TKI, imatinib, in 2000, the 10-year general survival (OS) trajectory for CML-CP has elevated from 20% to 80% (2). Presently, six TKIs are authorized for CP-CML therapy: first-generation TKI imatinib; second-generation (2G) TKIs nilotinib, dasatinib, and bosutinib; and third-generation (3G) TKIs ponatinib and asciminib. For almost all of CP-CML sufferers, imatinib is really helpful because the first-line (1L) remedy for long-term illness management (3). Imatinib is usually related to fewer cardiovascular and arterio-occlusive occasions in comparison with 2G TKIs (4–6). Nonetheless, because of varied causes, together with disease-related elements or the pursuit of a better and quicker treatment-free remission (TFR), some sufferers might go for a second-generation TKI as 1L therapy. However, there may be presently no proof indicating a survival benefit of second-generation TKIs over imatinib (7–9).
In main multicenter, section 3 medical trials evaluating imatinib to 2G TKIs in newly identified CML-CP, equivalent to dasatinib (DASISION), nilotinib (ENESTnd), and bosutinib (BFORE), larger charges of full cytogenetic response (CCyR) and main molecular response (MMR) have been noticed with 2G TKIs within the 1L setting (4, 5, 10). Dasatinib demonstrated CCyR and MMR charges at 12 months of 77% and 46%, respectively, versus 66% (P=0.007) and 28% (P=0.0001) with imatinib. Nilotinib 400 mg confirmed a confirmed MMR fee at 12 months of 43% versus 22% (P=0.0001) with imatinib. Bosutinib exhibited CCyR and MMR charges at 12 months of 77% and 47%, respectively, versus 66% (P=0.0075) and 37% (P=0.0200) with imatinib. Cumulative 5-year MR4.5 charges have been as follows: dasatinib 42% versus imatinib 33% (P=0.0251); nilotinib 52% versus imatinib 31% (P=0.0001); bosutinib 47.4% versus 36.6% (4–6).
Therapy failure might outcome from both major resistance, outlined as the shortcoming to attain goal molecular responses throughout the specified length, or secondary resistance, characterised by the lack of prior response. Intolerance is outlined as recurrent grade ≥ 3 hematological toxicity or ≥ 2 nonhematological toxicity requiring discontinuation regardless of dose discount (4). Discontinuation charges because of antagonistic occasions (AEs) have been reported as follows: IRIS (7%), DASISION (16%), ENESTnd (12%) (nilotinib 300mg twice each day), BFORE (25%), PACE (21%), and ASCEMBL (5.8%) (4–6, 11, 12). Every TKI has distinctive toxicity profiles, so exercising warning when choosing an acceptable TKI can enhance compliance and mitigate negative effects.
After real resistance to 2G TKIs, a stronger remedy is required. The selection ought to be based mostly on disease-specific elements equivalent to mutational profile, cytogenetics, threat profile, and antagonistic occasions of particular and prior TKI remedy. Present suggestions embody switching to a different 2G TKI or a 3G TKI, with plans for early allogeneic stem cell transplantation or enrollment in a medical trial if therapy milestones or deep molecular responses (DMRs) usually are not achieved or maintained (13–16). Nonetheless, knowledge on exact medical steering post-2G TKI failure, whether or not used as 1L or second line (2L), are restricted. This assessment will present insights into medical proof and steering, together with new therapeutics in medical trials, following 2G TKI failure because of real resistance.
Mechanisms of resistance to second era TKI
Resistance to remedy mostly arises from both novel mutations within the BCR::ABL1 gene, equivalent to mutations within the kinase area or overexpression/amplification of BCR::ABL1, disrupting TKI binding. Mutations account for resistance in roughly one-third of resistant CP sufferers. Resistance may also happen by way of non-BCR::ABL1 mechanisms, together with SRC kinases or elevated P-glycoprotein efflux pump exercise, clonal evolution, diminished ranges of human natural cation transporter (hoct1) resulting in decreased TKI inflow, or elevated ranges of the multi-drug exporter of the ATP binding cassette (17–21). Genetic aberrations in ASXL1 have been discovered to be considerably larger in TKI-resistant sufferers handled with imatinib, elevating considerations about attainable preexisting ASXL1 mutations within the BCR::ABL1-positive leukemic clone impacting the medical response to imatinib. Nonetheless, additional research are wanted to validate this correlation because of the restricted pattern measurement (22).
Mutations at prognosis are uncommon however can emerge in sufferers because of noncompliance and should develop resistance to TKI remedy (23–27), or after a number of sequential TKI therapies, related to decreased response and worse general survival (18, 28). Mutations often contain acquired level mutations within the BCR::ABL kinase area (18, 28). Complete-genome sequencing with the identification of mutated genes equivalent to ASXL1 and TP53 in CP-CML might maintain prognostic and predictive significance, requiring additional investigation in medical administration (29).
Sequential therapies with TKIs enhance the vulnerability to the emergence of compound mutations, with two paired mutations occurring in 76% of circumstances, and triple (10.6%) and quadruple (1.5%) mutations throughout the similar BCR::ABL1 allele. Sadly, these are often insensitive even to third-generation TKIs (30–32). Ponatinib, a high-affinity pan BCR-ABL1 inhibitor, can suppress all single mutants within the BCR::ABL1 area, together with T315I. Nonetheless, the emergence of compound mutations in a BCR::ABL1 allele, particularly these involving T315I (e.g., Y253H/T315I, E2455V/T315I), might confer ponatinib resistance, even at a excessive dose of 45mg as soon as a day (31, 33, 34). A medical consideration is the related mixture of asciminib and ponatinib, which seems efficient in overcoming compound mutations involving T315I and decreasing ponatinib toxicity (34).
Standards for remedy failure
Failure could be categorized as both true resistance or intolerance. Nonetheless, the main focus of this paper might be on true resistance to 2G TKIs. Throughout remedy for CML-CP, there are particular suggestions concerning reaching goal molecular responses at completely different time factors (3, 6, 12 months) by measuring BCR::ABL transcript ranges utilizing real-time reverse transcriptase polymerase chain response (RT-PCR), as outlined in worldwide requirements (IS) (35, 36).
The 2013 European Leukemia Internet (ELN) definition had completely different standards for failure to first- and second-line TKIs, with much less stringent directions after failing second-line remedy. Nonetheless, the 2020 ELN definition considers the presence of a mutation and failure to attain a BCR::ABL1IS ≤1% or CCyR at 12 months as therapy failure, encompassing these receiving second-line TKIs. The ELN 2020 standards are summarized in Desk 1 (37).
Desk 1 ELN 2020 definition of failure to 1L and 2L therapy (37).
As usually acknowledged, second-generation TKIs obtain quicker charges of CCyR at early time factors in comparison with imatinib. Due to this fact, making use of ELN 2020 standards to the usage of second-generation TKIs as preliminary remedy in CML-CP will not be optimum. Beforehand, research by Jabbour et al. and extra just lately by Sasaki et al. have prompt that sufferers on 2G TKIs as frontline remedy had worse survival outcomes if an earlier swap to ponatinib or a novel TKI was not initiated when a 3-month BCR::ABL ≤10% and 6–12 month BCR::ABL1IS ≤1% weren’t achieved (38, 39). These tips set up therapy change targets to mitigate the danger of illness development.
Therapy failure might outcome from both major resistance, outlined as the shortcoming to attain goal molecular responses throughout the allotted length (Desk 1), or secondary resistance, characterised by the lack of prior response. The lack of CHR or CCyR necessitates a remedy swap, however the lack of MMR throughout the context of sustained CCyR permits for much less exact interpretation (21, 40).
Therapeutic choices after resistance to first-line second-generation TKI and outcomes
Whereas imatinib is taken into account the most secure choice (41), it doesn’t successfully inhibit a number of BCR::ABL mutations (42), aside from the gatekeeper mutation T315I, which is delicate to ponatinib and asciminib (19, 21). By 5 years, 30–55% of sufferers handled with 2G TKIs obtain a 4.5 log discount (MR4.5, BCR::ABL1IS <0.0032% IS), in comparison with roughly 30% handled with imatinib (4, 5). Though 2G and 3G TKIs have benefits over imatinib in reaching a quicker and deeper response, there may be presently no knowledge confirming larger charges of remedy (15, 37, 42).
Roughly 50% of sufferers with CML-CP handled with imatinib will swap remedy inside 5 years, in comparison with 30–40% when handled with frontline 2G TKI. Amongst these, practically 15%-25% change because of true resistance to imatinib related to the T315I mutation, whereas solely 5–7% are because of intolerance (4, 5, 43). At 5 years, the charges of resistance for nilotinib (ENESTend), dasatinib (DASISION), and bosutinib (BFORE) as first-line therapies are 23%, 26%, and 5.6%, respectively (4, 5, 44–46). The outcomes of 2G TKI as first-line remedy are outlined in Desk 2.
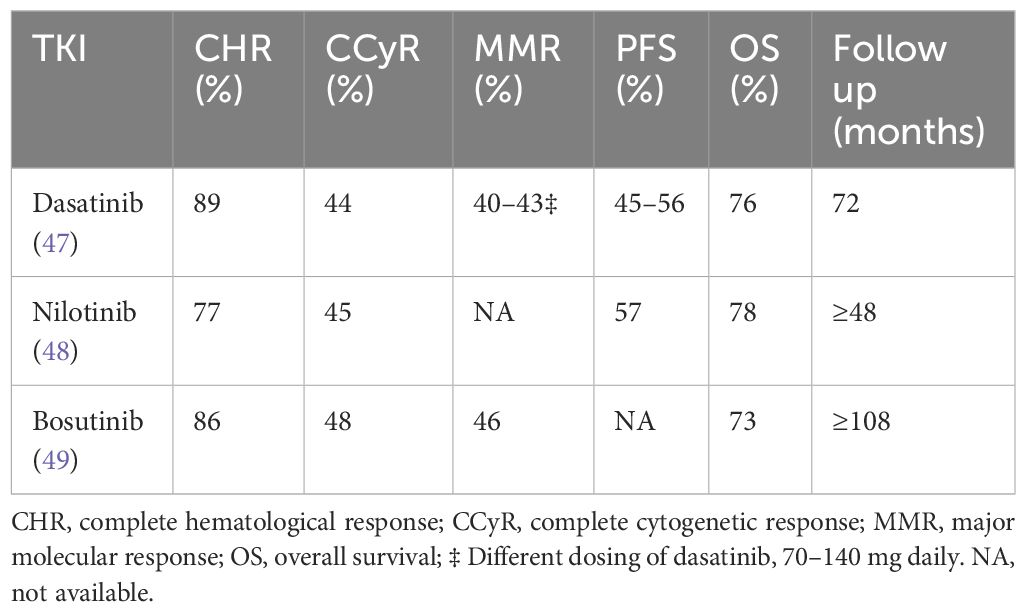
Desk 2 Outcomes of 2G TKI publish imatinib failure.
A minority of sufferers are immune to second-generation TKIs within the first-line setting and signify a inhabitants with a poor prognosis requiring a swap to different remedy. Failing a 2G TKI within the first-line setting is antagonistic in comparison with failing it within the second-line setting (21). Suppliers usually select 2G TKIs as first-line remedy as they supply larger charges of full CHR, CCyR, and MMR and are extra tolerable than high-dose imatinib (50–52).
Though there are not any potential trials and the affected person numbers are low, the charges of CCyR after failure of imatinib and dasatinib have been 27% and 20%, respectively, with nilotinib and bosutinib when used as third-line remedy, however have been larger with sequential ponatinib at 54%. When sufferers failed imatinib and nilotinib, the CCyR charges have been 25–26% with third-line remedy with dasatinib or bosutinib, whereas they have been 67% when switched to ponatinib. Comparable outcomes have been noticed in sufferers who failed a 2G TKI and switched to an alternate 2G TKI, leading to CCyR charges of twenty-two–26%, in comparison with 60% with ponatinib, together with T315I and non-T315I mutated sufferers (53, 54). Therefore, an alternate 2G TKI has restricted worth after resistance to a different 2G TKI within the absence of mutations, and few sufferers remained on therapy, indicating appreciable failure throughout research (55–60).
In a retrospective research of 62 sufferers with a median follow-up of 14 months, handled with fourth-line bosutinib post-failure to first-generation and remaining 2G TKIs, the chance of reaching and sustaining a CCyR and MMR was 25% and 24%, respectively. This quantity additional decreased to 14% to attain an MMR if sufferers weren’t in a CCyR on the time of beginning bosutinib (61).
Not too long ago, Kantarjian et al. demonstrated sustained excessive response and survival outcomes with ponatinib in sufferers immune to 2G TKIs, no matter T315I standing, enrolled within the PACE (Ponatinib Philadelphia chromosome-positive acute lymphoblastic leukemia and CML Analysis) and OPTIC (Optimizing Ponatinib Therapy in CP-CML) research. The progression-free survival (PFS) and general survival (OS) have been 68% and 85% within the PACE research, and 80% and 91% within the OPTIC research (62).
Due to this fact, within the case of resistance to a 2G TKI because of a selected mutation, different 2G TKIs might be thought-about. As an example, following resistance to dasatinib, nilotinib, or bosutinib might be choices relying on particular mutations, affected person comorbidities, compliance, drug-drug interactions, and prior antagonistic results. Nonetheless, in accordance with ELN 2020 tips, an earlier use of ponatinib ought to be thought-about in all eligible sufferers with out important heart problems, as they’re twice as more likely to obtain a CCyR when handled with ponatinib than with one other 2G TKI (62–65).
A number of elements have to be assessed for resistance to a 2G TKI, however mutational evaluation ought to be carried out primarily, and discussions concerning discovering an appropriate donor ought to be initiated. Subsequent-generation sequencing (NGS) is a extra delicate method than Sanger sequencing and might detect low-level mutations and compound mutations. Nonetheless, resistance to TKIs might not solely be because of low-level mutations and doesn’t information TKI choice except it includes T315I, which necessitates ponatinib or a better dose of asciminib (66). Detecting compound mutations, particularly Y253H/T315I and E2455V/T315I, ought to immediate a seek for a donor for allogeneic stem cell transplantation (30, 67, 68).
Cross tolerance is rare, and negative effects often change upon switching remedy, apart from myelosuppression, which may persist throughout TKIs (69–71). Nonetheless, sufferers who show failure to a number of TKIs and swap to an alternate 2G TKI might not expertise excessive response charges, and if achieved, the response shouldn’t be often sturdy (53–55). Reaching a CCyR at three months is independently related to event-free survival (EFS) and OS; therefore, in sufferers who usually are not candidates for transplantation, sustaining a CCyR with completely different TKIs might be a therapeutic aim relatively than aiming for MMR or a deeper response (72). Nonetheless, following resistance to a first- or second-generation TKI, a diminished CCyR is noticed.
Second line TKI: efficacy and outcomes
The controversy over one of the best technique for preliminary remedy ranges from beginning with a 2G TKI for a faster and extra profound response to switching to a 2G TKI after an insufficient response to imatinib. MMR is usually considered a surrogate for survival, and utilizing 2G TKIs as preliminary remedy has not demonstrated enhancements in general survival (OS), progression-free survival (PFS), or treatment-free remission (TFR) (7, 62, 73–75).
Whereas imatinib is often used worldwide because the first-line TKI, an rising variety of physicians are selecting 2G TKIs as first-line remedy to attain a quicker and deeper remission, with the intention of reaching TFR. Nonetheless, TFR is just thought-about acceptable if sufferers obtain a MMR with sustained deep remission, usually outlined as a 4-log lower in BCR::ABL transcript ranges from a standardized baseline, similar to a PCR <0.01% on the worldwide scale (IS) (76, 77).
In a cohort of 113 sufferers, fewer than 10% achieved a CCyR at 3–6 months and finally attained a significant cytogenetic response (MCyR) at 12 months after receiving a 2G TKI (dasatinib/nilotinib) (78).
In sufferers with imatinib failure, the T315I mutation was reported in 10–27%, nevertheless, within the second-line setting, it was noticed in 9–53% (43). At present, FDA-approved therapy choices for the T315I mutation embody ponatinib, asciminib, omacetaxine (solely authorized within the USA), and allo-SCT (19, 33, 79). Olverembatinib (HQP1351) is in medical trials and has proven exercise towards T315I.
Therapy with 2G TKIs after imatinib failure may end up in excessive response charges and is a more practical choice in comparison with larger doses of imatinib (800mg each day) in reaching larger CCyR and MMR (50, 51, 80, 81). Desk 2 illustrates outcomes with second-line TKIs after imatinib resistance.
PACE and OPTIC research and real-world ponatinib knowledge
Ponatinib, a 3G TKI, is authorized for sufferers with the T315I mutation or these resistant or illiberal to not less than two TKIs in CML-CP (82, 83). Within the 5-year follow-up of the pivotal PACE trial (Ponatinib Philadelphia chromosome-positive acute lymphoblastic leukemia and CML Analysis), the place a closely pretreated cohort of sufferers resistant or illiberal to dasatinib or nilotinib, or with the T315I mutation, was enrolled, important findings have been noticed (84, 85). Out of 267 evaluable sufferers with CML-CP and after a median follow-up of 56.8 months and median length of therapy of 32.1 months, 144 (54%) achieved a CCyR, 108 (40%) achieved an MMR, and 64 (24%) achieved MR4.5. Of those that achieved an MCyR at 12 months and an MMR at any time, 82% and 59% of sufferers, respectively, maintained responses at 5 years. The median instances to MCyR, CCyR, and MMR amongst those that achieved the response have been 2.8, 2.9, and 5.5 months, respectively. The Kaplan-Meier estimated PFS and OS at 5 years have been 53% and 73%, respectively (82).
To higher decide the optimum dose of ponatinib whereas balancing efficiency and security, the section 2 open-label OPTIC research (Optimizing Ponatinib Therapy in CP-CML) was performed (NCT02467270), the place sufferers have been randomized to obtain both ponatinib at 45 mg each day (cohort A), 30 mg each day (cohort B), or 15 mg each day (cohort C). Preliminary analyses confirmed various charges of reaching BCR::ABL1IS ≤ 1% (MMR) at 12 months throughout the cohorts (84, 85). On the latest 3-year follow-up replace, MMR at 36 months was noticed in several percentages throughout the cohorts (86). Opposed occasions occurred in various percentages throughout the cohorts, with grade ≥3 antagonistic occasions reported in a smaller subset. Discontinuations because of treatment-emergent antagonistic occasions occurred in differing percentages throughout the cohorts, with a minimal variety of deaths reported (12, 84, 86).
Current knowledge from the Belgian registry on 33 CML-CP sufferers beforehand handled with not less than two TKIs confirmed promising outcomes with ponatinib, albeit with some incidence of remedy discontinuation because of negative effects (87). Equally, real-life expertise from Italy on treating sufferers with ponatinib demonstrated favorable responses but additionally highlighted remedy discontinuation charges because of resistance or intolerance (88).
Within the US registry for CML-CP sufferers receiving ponatinib, varied beginning doses have been noticed, with preferences and proposals outlined by ELN 2020 tips based mostly on cardiovascular threat elements and resistance profiles (37, 89–91). Using aspirin as major thromboprophylaxis whereas on TKI stays unsure (92, 93).
Asciminib: a first-in-class allosteric inhibitor
Asciminib, a pioneering selective allosteric BCR-ABL1 inhibitor, represents a definite mechanism of motion in comparison with presently obtainable TKIs. FDA approval in October 2021 for third-line use or in sufferers harboring the T315I mutation underscores its significance (82, 83). By mimicking the myristoyl peptide, asciminib exactly targets the ABL Myristoyl Pocket (STAMP inhibitor), thereby restoring the inactive type of the kinase in the course of the 9;22 translocation with out affecting the ATP binding website. This distinctive mechanism grants asciminib exercise towards varied ATP website resistance mutations, together with the gatekeeper T315I mutation, catalytic website, and P-loop mutation (excluding F359) (19, 94, 95).
Asciminib’s efficacy was initially explored within the section 1 CABL001X2101 trial, the place it was assessed as monotherapy or together with nilotinib or dasatinib in CML-CP or CML-AP as third-line remedy or within the second line for T315I mutation. Outcomes from the monotherapy cohort of 150 sufferers demonstrated promising outcomes, with important proportions reaching MMRs at varied time factors (19). Subsequent up to date outcomes from 115 sufferers, after practically 4 years of follow-up, revealed continued efficacy, with a substantial proportion sustaining MMRs and MR4s (96).
Widespread grade ≥3 antagonistic occasions included elevated pancreatic enzymes, thrombocytopenia, hypertension, and neutropenia, whereas musculoskeletal ache, higher respiratory tract an infection, and fatigue have been frequent all-grade antagonistic occasions (96).
Moreover, an expanded cohort of the section 1 research evaluated asciminib in 52 T315I-positive CML-CP sufferers at an escalated dose of 200mg BID, displaying notable MMR charges and a manageable security profile (19, 97).
In a subgroup evaluation of closely pretreated sufferers, asciminib monotherapy demonstrated effectiveness in reaching MMRs, MR4s, and MR4.5s, with a positive security profile (96, 98).
These promising section 1 outcomes paved the way in which for the ASCEMBL research, a section 3 trial evaluating asciminib to bosutinib in CML-CP sufferers who had skilled lack of efficacy or intolerance to ≥2 prior TKIs. Outcomes from this research highlighted the superior efficacy of asciminib over bosutinib, with larger MMR charges and fewer antagonistic occasions resulting in therapy discontinuation (11, 99).
Actual-world expertise with asciminib throughout varied nations has additional supported its efficacy within the third-line setting, with important proportions of sufferers reaching MMRs, even amongst these with prior ponatinib publicity (100–104).
Asciminib versus ponatinib, the higher drug?
Ponatinib and high-dose asciminib show comparable efficacy within the context of the T315I mutation, as noticed within the OPTIC and ASCEMBL trials, the place every TKI was assessed as a third-line choice. Ponatinib stands out as the popular selection for sufferers with the F359 mutation (which is immune to asciminib) and people with BCR::ABL >10% IS. Notably, within the OPTIC research, sufferers within the 45mg ponatinib group with >10% BCR::ABL achieved a better MMR fee at 3 years in comparison with these on asciminib at 24 weeks. Nonetheless, the longer follow-up length with OPTIC warrants consideration (11, 84, 85). Conversely, Asciminib boasts a positive vascular or cardiovascular security profile and could also be favored over ponatinib in sufferers with T315I mutation and important vascular illness. This choice may evolve with accumulating long-term asciminib knowledge. Asciminib may be most popular in sufferers illiberal to earlier 1G or 2G TKIs however who’ve achieved molecular response, as demonstrated within the ASCEMBL trial (105).
Compound mutations pose resistance to each TKIs. Given the absence of a direct head-to-head medical trial evaluating the efficacy and security of ponatinib and asciminib, the optimum remedy resolution ought to be individualized based mostly on affected person comorbidities and medical judgment.
Different therapeutic choices
Omacetaxine mepesuccinate is a protein translation inhibitor that doesn’t goal the BCR-ABL kinase area however induces apoptosis in BCR::ABL1 optimistic cells by downregulating MCL-1. It’s efficient towards the T315I mutation and has been FDA-approved and obtainable within the USA since 2012 for sufferers resistant or illiberal to ≥ 2 TKIs, together with these with the T315I mutation (106, 107).
In a research involving 76 closely pretreated evaluable sufferers with CML-CP, omacetaxine was administered as induction remedy at 1.25mg/m² BID subcutaneously for as much as 14 consecutive days each 28 days till hematological response, adopted by upkeep at 1.25mg/m² BID for as much as 7 days each 28-day cycle. The research reported that 53 sufferers (70%) achieved a CHR, 14 sufferers (18%) achieved an MCyR, and seven sufferers (9%) achieved a CCyR. Moreover, a partial cytogenetic response (PCyR) was achieved in 3.9% of sufferers, and a MCyR was achieved in 18.4%. Amongst 40 sufferers who had obtained 2 prior TKIs, 31 (78%) achieved a CHR, 10 (25%) an MCyR, and 5 (13%) a CCyR. Amongst 36 sufferers who had obtained 3 prior TKIs, 22 (61%) achieved a CHR, 4 (11%) an MCyR, and a pair of (6%) a CCyR. For the 22 sufferers with T315I mutations at baseline, 18 (82%) achieved a CHR, 5 (23%) an MCyR, and three (14%) a CCyR. In 35 sufferers with CML-AP, 14.3% achieved a significant hematologic response, and 11.3% achieved a CHR with no proof of leukemia in 2.9% (106, 108).
Whereas omacetaxine is usually well-tolerated and appropriate for long-term administration, it may well trigger extended and extreme myelosuppression. Hematological negative effects occurring in ≥ 5% of sufferers included bone marrow failure (11%), thrombocytopenia (11%), and febrile neutropenia (7%). Widespread non-hematological negative effects have been diarrhea (43%), nausea (38%), fatigue (30%), infections (26%), pyrexia (22%), headache (22%), asthenia (22%), and arthralgia (20%). The median OS for evaluable sufferers and for many who obtained greater than three cycles have been 40.3 and 49.3 months, respectively. The median PFS for evaluable sufferers and for many who obtained greater than three cycles of remedy have been 9.6 and 9.9 months, respectively. Because of its reasonable efficacy, with an general PFS of lower than 10 months and an OS of beneath 4 years, omacetaxine is reserved for sufferers who’re unable to make use of any of the obtainable TKIs and people who usually are not candidates for allogenic stem cell transplantation (108).
Newer therapies
Regardless of the big range of therapeutic choices for CML-CP, some sufferers stay resistant or illiberal to all obtainable TKIs, creating a necessity for the event of latest TKIs, significantly for third-line remedy and sufferers with T315I mutations.
One promising candidate is olverembatinib (HQP1351), a third-generation orally energetic BCR-ABL1 TKI efficient in CML no matter genotype. It accomplished section I and II trials involving 101 sufferers (86 with CML-CP and 15 with CML-AP). The median time from prognosis to the initiation of olverembatinib remedy was 6 years. Among the many sufferers, 63% had the T315I mutation, and 83% had obtained ≥2 strains of TKI remedy. After a median follow-up of 30 months, the CHR, CCyR, and MMR charges for CML-CP sufferers have been 97%, 62%, and 51%, respectively. For these with the T315I mutation, these charges have been 100%, 84%, and 72%, respectively. At three years, the PFS was 96.3% for CML-CP sufferers and 71.4% for these with CML-AP. Dosing was administered each different day for 28 days, with cohorts receiving 1–60mg. Thrombocytopenia of any grade and grade 3/4 was reported in 75.2% and 49.5% of sufferers, respectively. The commonest non-hematological negative effects have been grade 1/2 pores and skin hyperpigmentation and hypertriglyceridemia (109–111).
In 2023, the American Society of Hematology up to date the outcomes of the section 2 research, confirming olverembatinib’s efficacy in TKI-resistant CML-CP, together with T315I, in comparison with one of the best obtainable remedy (imatinib, nilotinib, and dasatinib) (112). Encouraging outcomes led to olverembatinib’s approval in China in November 2021 for treating grownup sufferers with TKI-resistant CML-CP and T315I-mutated CML-AP, and once more in November 2023 for treating grownup sufferers with CML-CP immune to and/or illiberal of first- and second-generation TKIs (113).
Present therapy choices on this particular setting are suboptimal. Potential medical trials of single-agent TKIs within the third-line setting are detailed in Desk 3 and Determine 1. Moreover, a number of medical trials are exploring mixtures of TKIs with different brokers focusing on non-BCR-ABL-mediated CML leukemia stem cell (LSC) resistance. CML LSCs usually are not depending on the kinase exercise of BCR-ABL1 and are usually not eradicated by TKIs (117, 118). Determine 2 supplies a schematic algorithm for managing CML-CP sufferers who fail 2G TKI remedy.
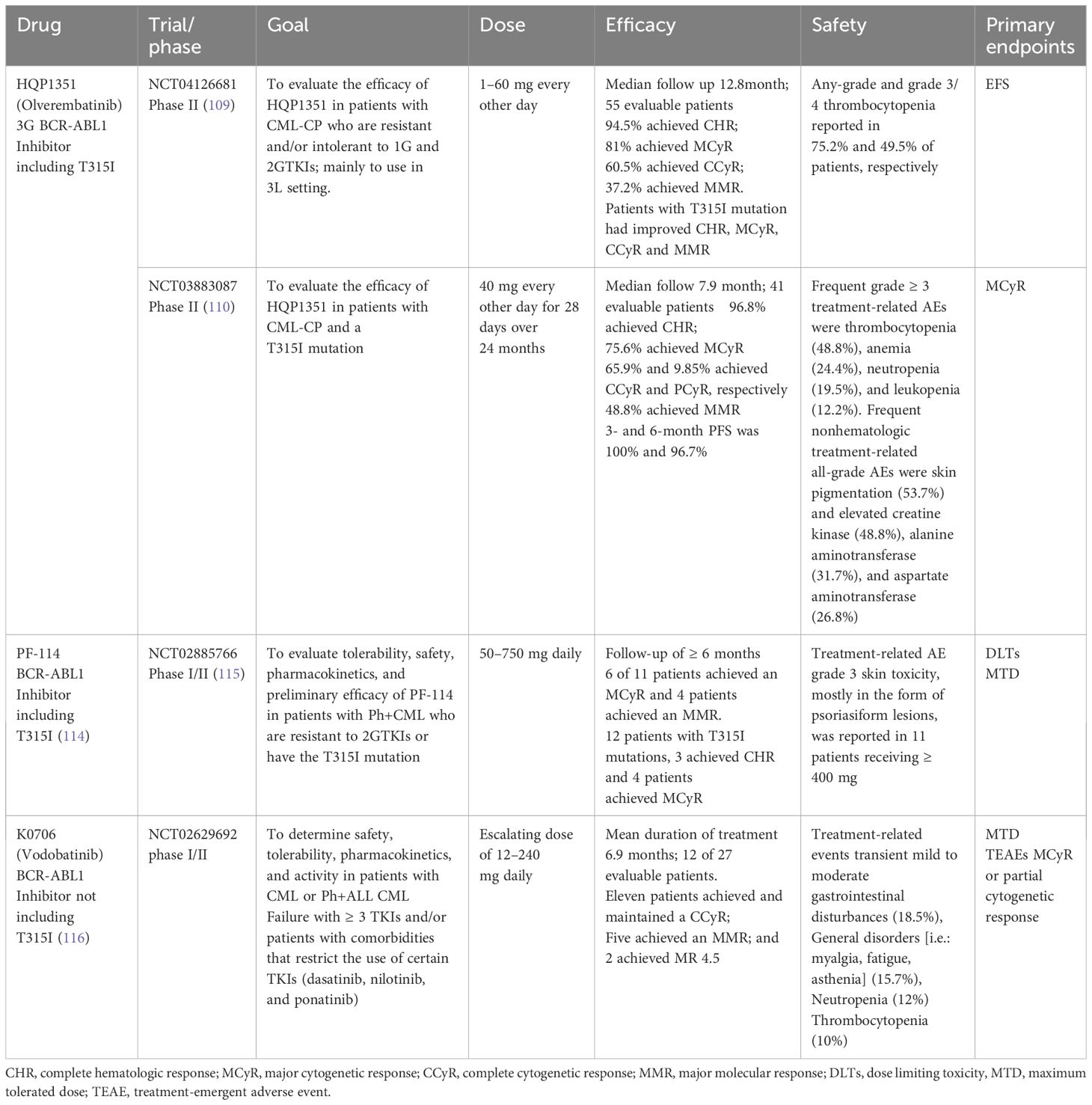
Desk 3 Ongoing medical trials for BCR-ABL focused therapies for CML in 3L+ context.
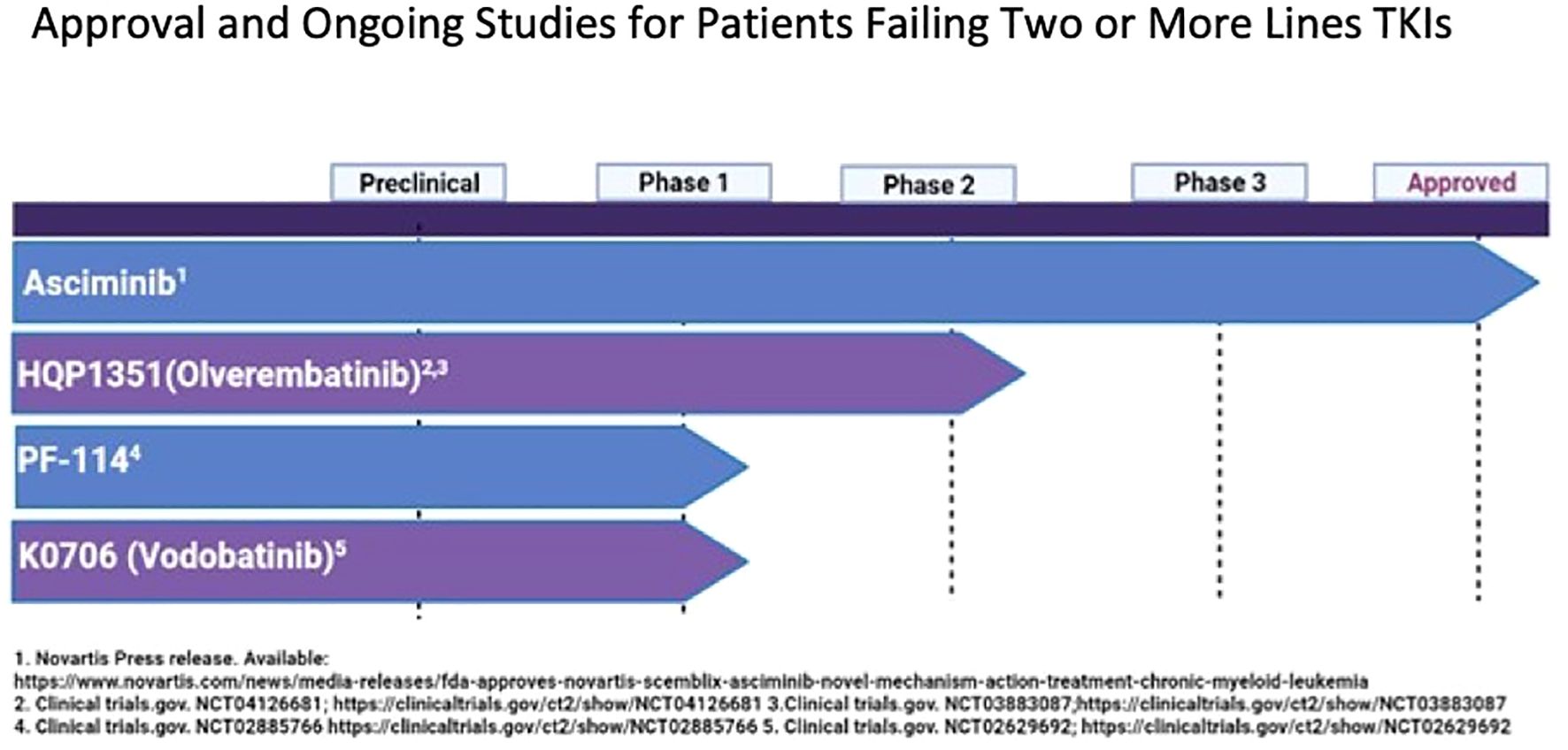
Determine 1 Approval and ongoing research for sufferers failing 2 or extra strains TKIs.
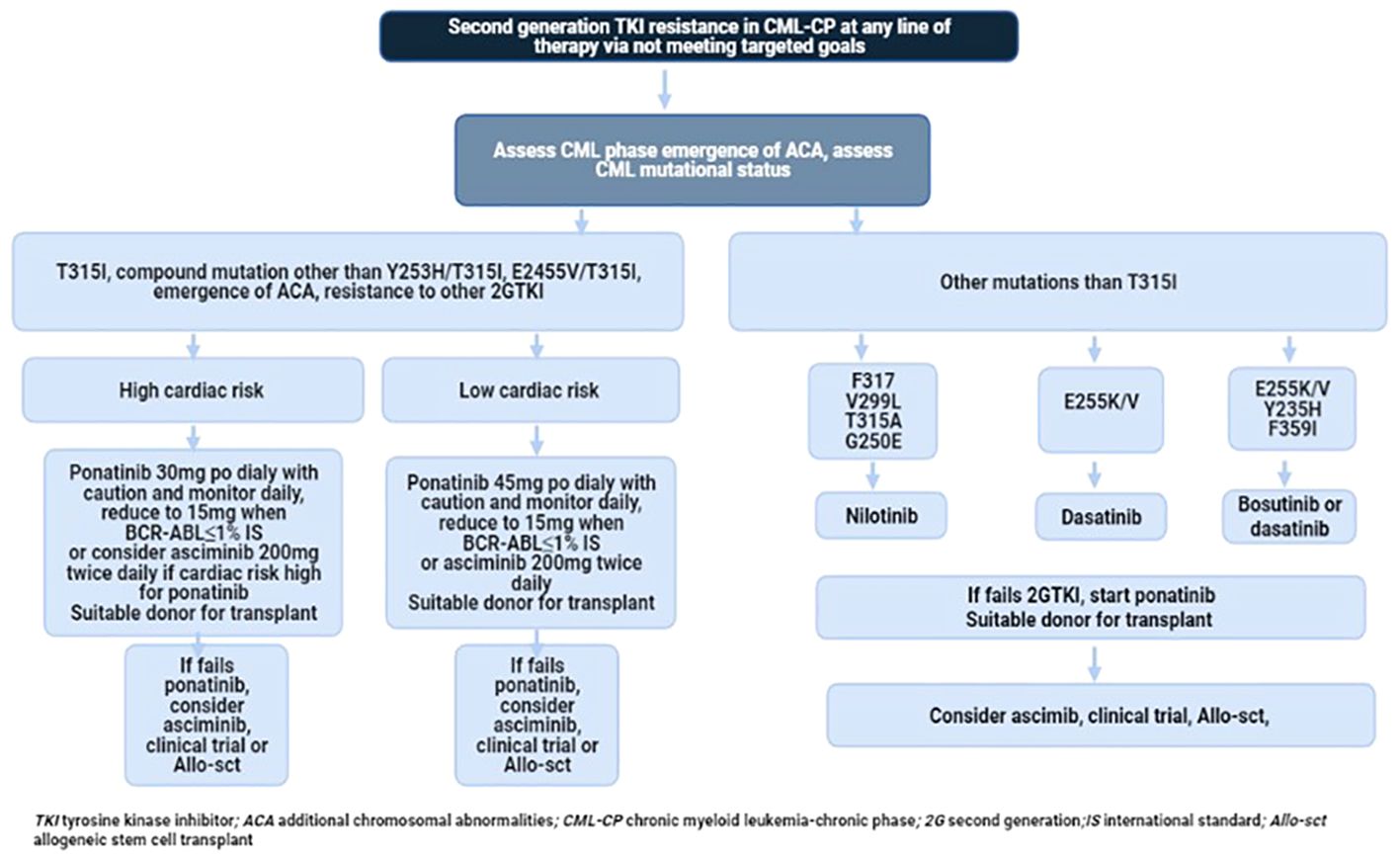
Determine 2 Advisable stream chart of administration in sufferers with CP-CML who developed resistance to 2G TKI.
Trying TFR in sufferers who exhibit resistance to 2G TKIs shouldn’t be presently really helpful, though it stays a extensively desired aim that’s untimely to undertake at this stage.
When ought to an allogeneic transplant (allo-SCT) be thought-about?
Allo-SCT holds important therapeutic implications because it represents a crucial boundary between TKI therapy and transplantation. Earlier than the period of TKIs like imatinib, allo-SCT was the one healing choice and stays essential at the moment. Delaying transplant till all TKI choices are exhausted is unfavorable, particularly for sufferers with compound mutations or excessive threat of extra chromosomal aberrations (e.g., isochromosome 12, advanced karyotype, trisomy 8, trisomy 19, monosomy 7, chromosome 3 abnormalities) (119).
Present ELN tips advocate contemplating allo-SCT for CML-CP sufferers resistant or illiberal to a second-line TKI or these with a T315I mutation (36, 37, 65). Additional research are wanted to know the implications of allo-SCT within the presence of somatic mutations equivalent to ASXL1 or TP53 (22, 29).
The Heart for Worldwide Blood and Marrow Analysis (CIBMTR) reported fewer than 300 transplants for CML-CP from 2014–2016. In comparison with TKI remedy, allo-SCT achieves larger leukemia-free survival however is related to practically 20% transplant-related mortality at one 12 months and decreased high quality of life because of transplant problems like graft-versus-host illness. The five-year cumulative incidence of relapse (CIR) was 18%, with most relapses occurring within the first-year post-transplant, and the five-year general survival (OS) was 68%. In 2020, CIBMTR reported fewer than 200 allotransplants for CML, primarily for accelerated and blast phases, whereas the European Bone Marrow Transplant (EBMT) registry reported practically 400 transplants for CML, with nearly half for CML-CP (120, 121). A latest Swedish research indicated three-year and five-year OS charges of roughly 85% and 96% for CML-CP, respectively, with a non-relapse mortality (NRM) of about 12% (122). Survival charges from varied transplant registries are outlined in Desk 4.
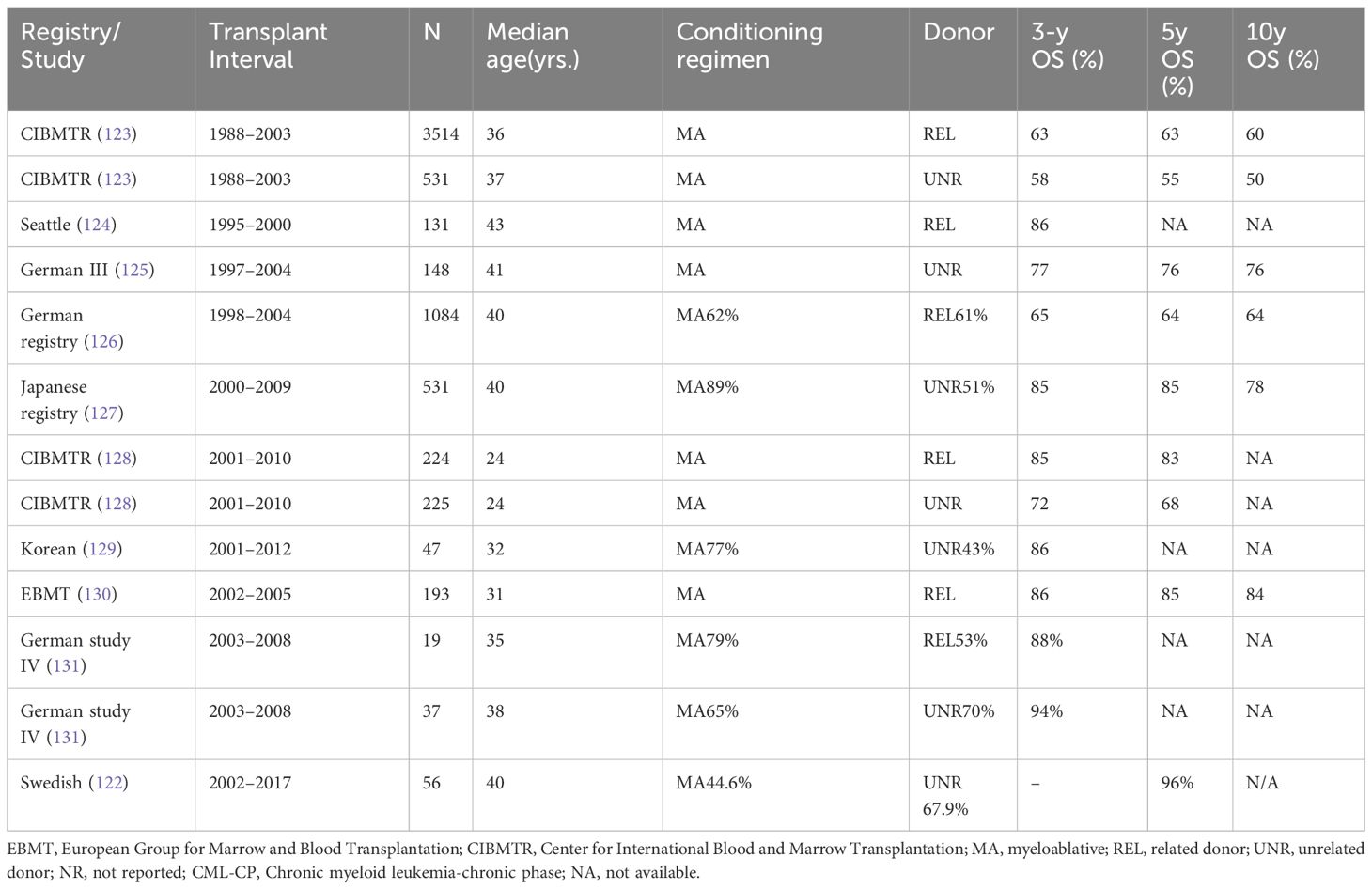
Desk 4 Total survival after allotransplant in CML-CP.
Advances in transplant strategies, together with the usage of matched associated donors, stopping early relapses with donor lymphocyte infusion (DLI), stopping post-transplant immunosuppression, and treating with TKIs post-transplant, have improved three-year OS to above 85% and 15-year leukemia-free survival (LFS) to 80% (131–135). Though late relapses are uncommon, the danger of relapse continues indefinitely (135).
The affect of TKI use earlier than and after transplant, in addition to the variety of TKIs used earlier than transplant, on post-transplant OS stays unclear (134, 136). An EBMT rating better than 2 persistently reveals an antagonistic affect on transplant outcomes and serves as a vital device for guiding transplant selections (125, 133, 137). Nonetheless, not all sufferers who fail TKI remedy are transplant candidates, particularly older sufferers who might require reduced-intensity pre-transplant conditioning, which will increase relapse threat (138). Due to this fact, the choice to proceed with a transplant within the continual section is advanced, and early consideration for medical trials ought to be optimized for sufferers not deemed transplant candidates.
Conclusion
Regardless of developments and a variety of therapy choices for CML-CP, 30–50% of sufferers expertise failure with frontline imatinib inside 5 years (123). With newer therapies in improvement primarily focusing on the ATP-competitive BCR-ABL1, there ought to be a better deal with strategically sequencing the obtainable TKIs to optimize response and decrease the emergence of mutations and resistance. Asciminib has proven promising outcomes and might tackle a few of these unmet wants. Moreover, different pathways, together with JAK/STAT, mTOR, and immune signaling, are promising potential targets for CML. Sadly, some sufferers could also be unable to obtain a second-generation TKI, ponatinib, or endure allo-HSCT and can also be ineligible for medical trials. In such circumstances, interferon alpha might be a viable choice.
Creator contributions
BG: Conceptualization, Information curation, Formal evaluation, Investigation, Venture administration, Writing – authentic draft, Writing – assessment & modifying. KC: Information curation, Validation, Writing – authentic draft, Writing – assessment & modifying. AR: Information curation, Validation, Visualization, Writing – authentic draft, Writing – assessment & modifying.
Funding
The creator(s) declare that no monetary help was obtained for the analysis, authorship, and/or publication of this text.
Battle of curiosity
The authors declare that the analysis was performed within the absence of any industrial or monetary relationships that might be construed as a possible battle of curiosity.
Writer’s notice
All claims expressed on this article are solely these of the authors and don’t essentially signify these of their affiliated organizations, or these of the writer, the editors and the reviewers. Any product which may be evaluated on this article, or declare which may be made by its producer, shouldn’t be assured or endorsed by the writer.
References
1. Bower H, Björkholm M, Dickman PW, Höglund M, Lambert PC, Andersson TM. Life expectancy of sufferers with continual myeloid leukemia approaches the life expectancy of the final inhabitants. J Clin Oncol. (2016) 34:2851–7. doi: 10.1200/JCO.2015.66.2866
PubMed Summary | CrossRef Full Textual content | Google Scholar
2. Gambacorti-Passerini C, Antolini L, Mahon FX, Guilhot F, Deininger M, Fava C, et al. Multicenter unbiased evaluation of outcomes in continual myeloid leukemia sufferers handled with imatinib. J Natl Most cancers Inst. (2011) 103:553–61. doi: 10.1093/jnci/djr060
PubMed Summary | CrossRef Full Textual content | Google Scholar
3. Hehlmann R, Müller MC, Lauseker M, Hanfstein B, Fabarius A, Schreiber A, et al. Deep molecular response is reached by the vast majority of sufferers handled with imatinib, predicts survival, and is achieved extra rapidly by optimized high-dose imatinib: outcomes from the randomized CML-study IV. J Clin Oncol. (2014) 32:415–23. doi: 10.1200/JCO.2013.49.9020
PubMed Summary | CrossRef Full Textual content | Google Scholar
4. Cortes JE, Saglio G, Kantarjian HM, Baccarani M, Mayer J, Boqué C, et al. Last 5-year research outcomes of DASISION: the dasatinib versus imatinib research in treatment-naïve continual myeloid leukemia sufferers trial. J Clin Oncol. (2016) 34:2333–40. doi: 10.1200/JCO.2015.64.8899
PubMed Summary | CrossRef Full Textual content | Google Scholar
5. Hochhaus A, Saglio G, Hughes TP, Larson RA, Kim DW, Issaragrisil S, et al. Lengthy-term advantages and dangers of frontline nilotinib vs imatinib for continual myeloid leukemia in continual section: 5-year replace of the randomized ENESTnd trial. Leukemia. (2016) 30:1044–54. doi: 10.1038/leu.2016.5
PubMed Summary | CrossRef Full Textual content | Google Scholar
6. Brümmendorf TH, Cortes JE, Milojkovic D, Gambacorti-Passerini C, Clark RE, le Coutre P, et al. Bosutinib versus imatinib for newly identified continual section continual myeloid leukemia: ultimate outcomes from the BFORE trial. Leukemia. (2022) 36:1825–33. doi: 10.1038/s41375-022-01589-y
PubMed Summary | CrossRef Full Textual content | Google Scholar
7. Baccarani M, Abruzzese E, Accurso V, Albano F, Annunziata M, Barulli S, et al. Managing continual myeloid leukemia for treatment-free remission: a proposal from the GIMEMA CML WP. Blood Adv. (2019) 3:4280–90. doi: 10.1182/bloodadvances.2019000865
PubMed Summary | CrossRef Full Textual content | Google Scholar
9. Deininger MW, Shah NP, Altman JK, Berman E, Bhatia R, Bhatnagar B, et al. Persistent myeloid leukemia, model 2.2021, NCCN medical follow tips in oncology. J Natl Compr Canc Netw. (2020) 18:1385–415. doi: 10.6004/jnccn.2020.0047
PubMed Summary | CrossRef Full Textual content | Google Scholar
10. Cortes JE, Gambacorti-Passerini C, Deininger MW, Mauro MJ, Chuah C, Kim DW, et al. Bosutinib versus imatinib for newly identified continual myeloid leukemia: outcomes from the randomized BFORE trial. J Clin Oncol. (2018) 36:231–7. doi: 10.1200/JCO.2017.74.7162
PubMed Summary | CrossRef Full Textual content | Google Scholar
11. Réa D, Mauro MJ, Boquimpani C, Minami Y, Lomaia E, Voloshin S, et al. A section 3, open-label, randomized research of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or extra prior TKIs. Blood. (2021) 138:2031–41. doi: 10.1182/blood.2020009984
PubMed Summary | CrossRef Full Textual content | Google Scholar
12. Cortes JE, Kim DW, Pinilla-Ibarz J, le Coutre PD, Paquette R, Chuah C, et al. Ponatinib efficacy and security in Philadelphia chromosome-positive leukemia: ultimate 5-year outcomes of the section 2 PACE trial. Blood. (2018) 132:393–404. doi: 10.1182/blood-2016-09-739086
PubMed Summary | CrossRef Full Textual content | Google Scholar
13. Baccarani M, Castagnetti F, Gugliotta G, Rosti G. A assessment of the European LeukemiaNet suggestions for the administration of CML. Ann Hematol. (2015) 94 Suppl 2:S141–7. doi: 10.1007/s00277-015-2322-2
PubMed Summary | CrossRef Full Textual content | Google Scholar
14. Fava C, Saglio G. The biology of CML helps second-generation TKIs as frontline therapy. Clin Adv Hematol Oncol. (2017) 15:302–7.
15. Saglio G, Jabbour E. First-line remedy for continual section CML: choosing the optimum BCR-ABL1-targeted TKI. Leuk Lymphoma. (2018) 59:1523–38. doi: 10.1080/10428194.2017.1379074
PubMed Summary | CrossRef Full Textual content | Google Scholar
16. Lee SG, Lipton JH. The whole lot previous is new once more: the case for imatinib as frontline remedy in 2017. Clin Adv Hematol Oncol. (2017) 15:302–5.
17. Gorre ME, Mohammed M, Ellwood Okay, Hsu N, Paquette R, Rao PN, et al. Scientific resistance to STI-571 most cancers remedy attributable to BCR-ABL gene mutation or amplification. Science. (2001) 293:876–80. doi: 10.1126/science.1062538
PubMed Summary | CrossRef Full Textual content | Google Scholar
18. Cortes J, Jabbour E, Kantarjian H, Yin CC, Shan J, O’Brien S, et al. Dynamics of BCR-ABL kinase area mutations in continual myeloid leukemia after sequential therapy with a number of tyrosine kinase inhibitors. Blood. (2007) 110:4005–11. doi: 10.1182/blood-2007-03-080838
PubMed Summary | CrossRef Full Textual content | Google Scholar
19. Hughes TP, Mauro MJ, Cortes JE, Minami H, Rea D, DeAngelo DJ, et al. Asciminib in continual myeloid leukemia after ABL kinase inhibitor failure. N Engl J Med. (2019) 381:2315–26. doi: 10.1056/NEJMoa1902328
PubMed Summary | CrossRef Full Textual content | Google Scholar
20. Loscocco F, Visani G, Galimberti S, Curti A, Isidori A. BCR-ABL unbiased mechanisms of resistance in continual myeloid leukemia. Entrance Oncol. (2019) 9:939. doi: 10.3389/fonc.2019.00939
PubMed Summary | CrossRef Full Textual content | Google Scholar
21. Milojkovic D, Apperley J. Mechanisms of resistance to imatinib and second-generation tyrosine inhibitors in continual myeloid leukemia. Clin Most cancers Res. (2009) 15:7519–27. doi: 10.1158/1078-0432.CCR-09-1068
PubMed Summary | CrossRef Full Textual content | Google Scholar
22. Machnicki MM, Pepek M, Solarska I, Niesiobedzka-Krezel J, Seferynska I, Gora Tybor J, et al. ASXL1 mutations detectable at prognosis might predict response to imatinib in sufferers with continual myeloid leukemia. Blood. (2019) 134:4148–8. doi: 10.1182/blood-2019-129834
23. Branford S, Rudzki Z, Walsh S, Parkinson I, Grigg A, Szer J, et al. Detection of BCR-ABL mutations in sufferers with CML handled with imatinib is nearly all the time accompanied by medical resistance, and mutations within the ATP phosphate-binding loop (P-loop) are related to a poor prognosis. Blood. (2003) 102:276–83. doi: 10.1182/blood-2002-09-2896
PubMed Summary | CrossRef Full Textual content | Google Scholar
24. Soverini S, Martinelli G, Rosti G, Bassi S, Amabile M, Poerio A, et al. ABL mutations in late continual section continual myeloid leukemia sufferers with up-front cytogenetic resistance to imatinib are related to a better probability of development to blast disaster and shorter survival: a research by the GIMEMA Working Get together on Persistent Myeloid Leukemia. J Clin Oncol. (2005) 23:4100–9. doi: 10.1200/JCO.2005.05.531
PubMed Summary | CrossRef Full Textual content | Google Scholar
25. Soverini S, Colarossi S, Gnani A, Rosti G, Castagnetti F, Poerio A, et al. Contribution of ABL kinase area mutations to imatinib resistance in several subsets of Philadelphia-positive sufferers: by the GIMEMA Working Get together on Persistent Myeloid Leukemia. Clin Most cancers Res. (2006) 12:7374–9. doi: 10.1158/1078-0432.CCR-06-1516
PubMed Summary | CrossRef Full Textual content | Google Scholar
26. Khorashad JS, de Lavallade H, Apperley JF, Milojkovic D, Reid AG, Bua M, et al. Discovering of kinase area mutations in sufferers with continual section continual myeloid leukemia responding to imatinib might determine these at excessive threat of illness development. J Clin Oncol. (2008) 26:4806–13. doi: 10.1200/JCO.2008.16.9953
PubMed Summary | CrossRef Full Textual content | Google Scholar
27. Larson RA, Druker BJ, Guilhot F, O’Brien SG, Riviere GJ, Krahnke T, et al. Imatinib pharmacokinetics and its correlation with response and security in chronic-phase continual myeloid leukemia: a subanalysis of the IRIS research. Blood. (2008) 111:4022–8. doi: 10.1182/blood-2007-10-116475
PubMed Summary | CrossRef Full Textual content | Google Scholar
28. Soverini S, Gnani A, Colarossi S, Castagnetti F, Abruzzese E, Paolini S, et al. Philadelphia-positive sufferers who already harbor imatinib-resistant Bcr-Abl kinase area mutations have a better probability of growing extra mutations related to resistance to second- or third-line tyrosine kinase inhibitors. Blood. (2009) 114:2168–71. doi: 10.1182/blood-2009-01-197186
PubMed Summary | CrossRef Full Textual content | Google Scholar
29. Menezes J, Salgado RN, Acquadro F, Gómez-López G, Carralero MC, Barroso A, et al. ASXL1, TP53 and IKZF3 mutations are current within the continual section and blast disaster of continual myeloid leukemia. Blood Most cancers J. (2013) 3:e157. doi: 10.1038/bcj.2013.54
PubMed Summary | CrossRef Full Textual content | Google Scholar
30. Soverini S, De Benedittis C, Machova Polakova Okay, Brouckova A, Horner D, Iacono M, et al. Unraveling the complexity of tyrosine kinase inhibitor-resistant populations by ultra-deep sequencing of the BCR-ABL kinase area. Blood. (2013) 122:1634–48. doi: 10.1182/blood-2013-03-487728
PubMed Summary | CrossRef Full Textual content | Google Scholar
31. Zabriskie MS, Eide CA, Tantravahi SK, Vellore NA, Estrada J, Nicolini FE, et al. BCR-ABL1 compound mutations combining key kinase area positions confer medical resistance to ponatinib in Ph chromosome-positive leukemia. Most cancers Cell. (2014) 26:428–42. doi: 10.1016/j.ccr.2014.07.006
PubMed Summary | CrossRef Full Textual content | Google Scholar
32. Schmitt MW, Pritchard JR, Leighow SM, Aminov BI, Beppu L, Kim DS, et al. Single-molecule sequencing reveals patterns of preexisting drug resistance that counsel therapy methods in philadelphia-positive leukemias. Clin Most cancers Res. (2018) 24:5321–34. doi: 10.1158/1078-0432.CCR-18-0167
PubMed Summary | CrossRef Full Textual content | Google Scholar
33. O’Hare T, Shakespeare WC, Zhu X, Eide CA, Rivera VM, Wang F, et al. AP24534, a pan-BCR-ABL inhibitor for continual myeloid leukemia, potently inhibits the T315I mutant and overcomes mutation-based resistance. Most cancers Cell. (2009) 16:401–12. doi: 10.1016/j.ccr.2009.09.028
PubMed Summary | CrossRef Full Textual content | Google Scholar
34. Eide CA, Zabriskie MS, Savage Stevens SL, Antelope O, Vellore NA, Than H, et al. Combining the allosteric inhibitor asciminib with ponatinib suppresses emergence of and restores efficacy towards extremely resistant BCR-ABL1 mutants. Most cancers Cell. (2019) 36:431–443.e5. doi: 10.1016/j.ccell.2019.08.004
PubMed Summary | CrossRef Full Textual content | Google Scholar
35. Baccarani M, Cortes J, Pane F, Niederwieser D, Saglio G, Apperley J, et al. Persistent myeloid leukemia: an replace of ideas and administration suggestions of European LeukemiaNet. J Clin Oncol. (2009) 27:6041–51. doi: 10.1200/JCO.2009.25.0779
PubMed Summary | CrossRef Full Textual content | Google Scholar
36. Baccarani M, Deininger MW, Rosti G, Hochhaus A, Soverini S, Apperley JF, et al. European LeukemiaNet suggestions for the administration of continual myeloid leukemia: 2013. Blood. (2013) 122:872–84. doi: 10.1182/blood-2013-05-501569
PubMed Summary | CrossRef Full Textual content | Google Scholar
38. Jabbour E, et al. Entrance-line remedy with second-generation tyrosine kinase inhibitors in sufferers with early continual section continual myeloid leukemia: what’s the optimum response? J Clin Oncol. (2011) 29:4260–5. doi: 10.1200/JCO.2011.36.0693
PubMed Summary | CrossRef Full Textual content | Google Scholar
39. Sasaki Okay, Kantarjian HM, Issa GC, Garcia-Manero G, Kadia TM, et al. Affect of molecular response at particular timepoints in sufferers with newly identified continual myeloid leukemia handled with second era tyrosine kinase inhibitors. Blood. (2020) 136(Complement 1):42–44. doi: 10.1182/blood-2020-143023
40. Hochhaus A, La Rosée P. Imatinib remedy in continual myelogenous leukemia: methods to keep away from and overcome resistance. Leukemia. (2004) 18:1321–31. doi: 10.1038/sj.leu.2403426
PubMed Summary | CrossRef Full Textual content | Google Scholar
41. O’Hare T, Eide CA, Deininger MW. Bcr-Abl kinase area mutations, drug resistance, and the street to a remedy for continual myeloid leukemia. Blood. (2007) 110:2242–9. doi: 10.1182/blood-2007-03-066936
PubMed Summary | CrossRef Full Textual content | Google Scholar
43. Soverini S, Branford S, Nicolini FE, Talpaz M, Deininger MW, Martinelli G, et al. Implications of BCR-ABL1 kinase domain-mediated resistance in continual myeloid leukemia. Leuk Res. (2014) 38:10–20. doi: 10.1016/j.leukres.2013.09.011
PubMed Summary | CrossRef Full Textual content | Google Scholar
44. Kantarjian HM, Hochhaus A, Saglio G, De Souza C, Flinn IW, Stenke L, et al. Nilotinib versus imatinib for the therapy of sufferers with newly identified continual section, Philadelphia chromosome-positive, continual myeloid leukaemia: 24-month minimal follow-up of the section 3 randomised ENESTnd trial. Lancet Oncol. (2011) 12:841–51. doi: 10.1016/S1470-2045(11)70201-7
PubMed Summary | CrossRef Full Textual content | Google Scholar
45. Kantarjian HM, Shah NP, Cortes JE, Baccarani M, Agarwal MB, Undurraga MS, et al. Dasatinib or imatinib in newly identified chronic-phase continual myeloid leukemia: 2-year follow-up from a randomized section 3 trial (DASISION). Blood. (2012) 119:1123–9. doi: 10.1182/blood-2011-08-376087
PubMed Summary | CrossRef Full Textual content | Google Scholar
46. Kantarjian HM, Hughes TP, Larson RA, Kim DW, Issaragrisil S, le Coutre P, et al. Lengthy-term outcomes with frontline nilotinib versus imatinib in newly identified continual myeloid leukemia in continual section: ENESTnd 10-year evaluation. Leukemia. (2021) 35:440–53. doi: 10.1038/s41375-020-01111-2
PubMed Summary | CrossRef Full Textual content | Google Scholar
47. Shah NP, Guilhot F, Cortes JE, Schiffer CA, le Coutre P, Brümmendorf TH, et al. Lengthy-term consequence with dasatinib after imatinib failure in chronic-phase continual myeloid leukemia: follow-up of a section 3 research. Blood. (2014) 123:2317–24. doi: 10.1182/blood-2013-10-532341
PubMed Summary | CrossRef Full Textual content | Google Scholar
48. Giles FJ, le Coutre PD, Pinilla-Ibarz J, Larson RA, Gattermann N, Ottmann OG, et al. Nilotinib in imatinib-resistant or imatinib-intolerant sufferers with continual myeloid leukemia in continual section: 48-month follow-up outcomes of a section II research. Leukemia. (2013) 27:107–12. doi: 10.1038/leu.2012.181
PubMed Summary | CrossRef Full Textual content | Google Scholar
49. Brümmendorf TH, Cortes JE, Goh YT, Yilmaz M, Klisovic RB, Purcell S, et al. Bosutinib (BOS) for continual section (CP) continual myeloid leukemia (CML) after imatinib (IMA) failure: ≥8-y replace of a section I/II research. J Clin Oncol. (2020) 38-:7549–9.
50. Kantarjian H, Pasquini R, Lévy V, Jootar S, Holowiecki J, Hamerschlak N, et al. Dasatinib or high-dose imatinib for chronic-phase continual myeloid leukemia immune to imatinib at a dose of 400 to 600 milligrams each day: two-year follow-up of a randomized section 2 research (START-R). Most cancers. (2009) 115:4136–47. doi: 10.1002/cncr.24504
PubMed Summary | CrossRef Full Textual content | Google Scholar
51. Cortes JE, Kantarjian HM, Brümmendorf TH, Kim DW, Turkina AG, Shen ZX, et al. Security and efficacy of bosutinib (SKI-606) in continual section Philadelphia chromosome-positive continual myeloid leukemia sufferers with resistance or intolerance to imatinib. Blood. (2011) 118:4567–76. doi: 10.1182/blood-2011-05-355594
PubMed Summary | CrossRef Full Textual content | Google Scholar
52. Garcia-Gutierrez JV, Herrera P, Abalo LL. Affect of second-generation tyrosine kinase inhibitors as second line therapy for sufferers with continual myeloid. Am Soc Hematol. (2011) 118:3780. doi: 10.1182/blood.V118.21.3780.3780
53. Lipton JH, Shah D, Tongbram V, Sidhu M, Huang H, McGarry LJ, et al. Comparative efficacy amongst third line post-imatinib continual phase-chronic myeloid leukemia (CP-CML) sufferers after failure of dasatinib or nilotinib tyrosine kinase inhibitors. Blood. (2014) 124:4551–1. doi: 10.1182/blood.V124.21.4551.4551
54. Lipton JH, Bryden P, Sidhu MK, Huang H, McGarry LJ, Lustgarten S, et al. Comparative efficacy of tyrosine kinase inhibitor remedies within the third-line setting, for chronic-phase continual myelogenous leukemia after failure of second-generation tyrosine kinase inhibitors. Leuk Res. (2015) 39:58–64. doi: 10.1016/j.leukres.2014.10.005
PubMed Summary | CrossRef Full Textual content | Google Scholar
55. Garg RJ, Kantarjian H, O’Brien S, Quintás-Cardama A, Faderl S, Estrov Z, et al. Using nilotinib or dasatinib after failure to 2 prior tyrosine kinase inhibitors: long-term follow-up. Blood. (2009) 114:4361–8. doi: 10.1182/blood-2009-05-221531
PubMed Summary | CrossRef Full Textual content | Google Scholar
56. Giles FJ, Abruzzese E, Rosti G, Kim DW, Bhatia R, Bosly A, et al. Nilotinib is energetic in continual and accelerated section continual myeloid leukemia following failure of imatinib and dasatinib remedy. Leukemia. (2010) 24:1299–301. doi: 10.1038/leu.2010.110
PubMed Summary | CrossRef Full Textual content | Google Scholar
57. Ibrahim AR, Paliompeis C, Bua M, Milojkovic D, Szydlo R, Khorashad JS, et al. Efficacy of tyrosine kinase inhibitors (TKIs) as third-line remedy in sufferers with continual myeloid leukemia in continual section who’ve failed 2 prior strains of TKI remedy. Blood. (2010) 116:5497–500. doi: 10.1182/blood-2010-06-291922
PubMed Summary | CrossRef Full Textual content | Google Scholar
58. Cortes J, Quintas-Cardama A, Jabbour E, O’Brien S, Verstovsek S, Borthakur G, et al. The medical significance of reaching completely different ranges of cytogenetic response in sufferers with continual section continual myeloid leukemia after failure to front-line remedy: is full cytogenetic response the one fascinating endpoint? Clin Lymphoma Myeloma Leuk. (2011) 11:421–6. doi: 10.1016/j.clml.2011.06.009
PubMed Summary | CrossRef Full Textual content | Google Scholar
59. Ribeiro BF, Miranda ECM, de Albuquerque DulcinéiaM, Delamain MárciaT, Oliveira-Duarte G, Almeida MH, et al. Therapy with dasatinib or nilotinib in continual myeloid leukemia sufferers who failed to answer two beforehand administered tyrosine kinase inhibitors – a single middle expertise. Clinics. (2015) 70:550. doi: 10.6061/clinics/2015(08)04
PubMed Summary | CrossRef Full Textual content | Google Scholar
60. Lomaia E, Zaritskey A, Shuvavev V, Martynkevich I, Forminykh M, Ovsyannikova E, et al. Efficacy of tyrosine kinase inhibitors in third line remedy in continual section continual myeloid leukemia. Blood. (2015) 126:4051–1. doi: 10.1182/blood.V126.23.4051.4051
61. García-Gutiérrez V, Milojkovic D, Hernandez-Boluda JC, Claudiani S, Martin Mateos ML, Casado-Montero LF, et al. Security and efficacy of bosutinib in fourth-line remedy of continual myeloid leukemia sufferers. Ann Hematol. (2019) 98:321–30. doi: 10.1007/s00277-018-3507-2
PubMed Summary | CrossRef Full Textual content | Google Scholar
62. Kantarjian HM, Jabbour E, Deininger M, Abruzzese E, Apperley J, Cortes J, et al. Ponatinib after failure of second-generation tyrosine kinase inhibitor in resistant chronic-phase continual myeloid leukemia. Am J Hematol. (2022) 97:1419–26. doi: 10.1002/ajh.26686
PubMed Summary | CrossRef Full Textual content | Google Scholar
63. García-Gutiérrez V, Hernández-Boluda JC. Tyrosine kinase inhibitors obtainable for continual myeloid leukemia: efficacy and security. Entrance Oncol. (2019) 9:603. doi: 10.3389/fonc.2019.00603
PubMed Summary | CrossRef Full Textual content | Google Scholar
64. Hochhaus A, et al. Persistent myeloid leukaemia: ESMO Scientific Observe Pointers for prognosis, therapy and follow-up. Ann Oncol. (2017) 28:iv41–51. doi: 10.1093/annonc/mdx219
PubMed Summary | CrossRef Full Textual content | Google Scholar
66. Machova Polakova Okay, Kulvait V, Benesova A, Linhartova J, Klamova H, Jaruskova M, et al. Subsequent-generation deep sequencing improves detection of BCR-ABL1 kinase area mutations rising beneath tyrosine kinase inhibitor therapy of continual myeloid leukemia sufferers in continual section. J Most cancers Res Clin Oncol. (2015) 141:887–99. doi: 10.1007/s00432-014-1845-6
PubMed Summary | CrossRef Full Textual content | Google Scholar
67. Baer C, Kern W, Koch S, Nadarajah N, Schindela S, Meggendorfer M, et al. Extremely-deep sequencing results in earlier and extra delicate detection of the tyrosine kinase inhibitor resistance mutation T315I in continual myeloid leukemia. Haematologica. (2016) 101:830–8. doi: 10.3324/haematol.2016.145888
PubMed Summary | CrossRef Full Textual content | Google Scholar
68. Soverini S, Bavaro L, De Benedittis C, Martelli M, Iurlo A, Orofino N, et al. Potential evaluation of NGS-detectable mutations in CML sufferers with nonoptimal response: the NEXT-in-CML research. Blood. (2020) 135:534–41. doi: 10.1182/blood.2019002969
PubMed Summary | CrossRef Full Textual content | Google Scholar
69. Cortes JE, Hochhaus A, le Coutre PD, Rosti G, Pinilla-Ibarz J, Jabbour E, et al. Minimal cross-intolerance with nilotinib in sufferers with continual myeloid leukemia in continual or accelerated section who’re illiberal to imatinib. Blood. (2011) 117:5600–6. doi: 10.1182/blood-2010-11-318949
PubMed Summary | CrossRef Full Textual content | Google Scholar
70. Khoury HJ, Goldberg SL, Mauro MJ, Stone RM, Deininger MW, Bradley-Garelik MB, et al. Cross-intolerance with dasatinib amongst imatinib-intolerant sufferers with continual section continual myeloid leukemia. Clin Lymphoma Myeloma Leuk. (2016) 16:341–349.e1. doi: 10.1016/j.clml.2016.03.004
PubMed Summary | CrossRef Full Textual content | Google Scholar
71. Kobayashi Y, Sakamaki H, Fujisawa S, Ando Okay, Yamamoto Okay, Okada M, et al. Lack of non-hematological cross intolerance of dasatinib to imatinib in imatinib-intolerant sufferers with Philadelphia chromosome optimistic continual myeloid leukemia or acute lymphatic leukemia: a retrospective security evaluation. Int J Hematol. (2011) 93:745–9. doi: 10.1007/s12185-011-0864-1
PubMed Summary | CrossRef Full Textual content | Google Scholar
72. Jabbour E, Kantarjian H, Ghanem H, O’Brien S, Quintas-Cardama A, Garcia-Manero G, et al. The achievement of a 3-month full cytogenetic response to second-generation tyrosine kinase inhibitors predicts survival in sufferers with continual section continual myeloid leukemia after imatinib failure. Clin Lymphoma Myeloma Leuk. (2013) 13:302–6. doi: 10.1016/j.clml.2012.12.005
PubMed Summary | CrossRef Full Textual content | Google Scholar
73. Hehlmann R, Lauseker M, Saußele S, Pfirrmann M, Krause S, Kolb HJ, et al. Evaluation of imatinib as first-line therapy of continual myeloid leukemia: 10-year survival outcomes of the randomized CML research IV and affect of non-CML determinants. Leukemia. (2017) 31:2398–406. doi: 10.1038/leu.2017.253
PubMed Summary | CrossRef Full Textual content | Google Scholar
74. Hochhaus A, Larson RA, Guilhot F, Radich JP, Branford S, Hughes TP, et al. Lengthy-term outcomes of imatinib therapy for continual myeloid leukemia. N Engl J Med. (2017) 376:917–27. doi: 10.1056/NEJMoa1609324
PubMed Summary | CrossRef Full Textual content | Google Scholar
75. Jain P, Kantarjian H, Nazha A, O’Brien S, Jabbour E, Romo CG, et al. Early responses predict higher outcomes in sufferers with newly identified continual myeloid leukemia: outcomes with 4 tyrosine kinase inhibitor modalities. Blood. (2013) 121:4867–74. doi: 10.1182/blood-2013-03-490128
PubMed Summary | CrossRef Full Textual content | Google Scholar
76. Etienne G, Faberes C, Bauduer F, Adiko D, Lifermann F, Dagada C, et al. Relevance of treatment-free remission suggestions in continual section continual leukemia sufferers handled with frontline tyrosine kinase inhibitors. Most cancers Med. (2021) 10:3635–45. doi: 10.1002/cam4.3921
PubMed Summary | CrossRef Full Textual content | Google Scholar
77. Haddad FG, Sasaki Okay, Issa GC, Garcia-Manero G, Ravandi F, Kadia T, et al. Therapy-free remission in sufferers with continual myeloid leukemia following the discontinuation of tyrosine kinase inhibitors. Am J Hematol. (2022) 97:856–64. doi: 10.1002/ajh.26550
PubMed Summary | CrossRef Full Textual content | Google Scholar
78. Tam CS, Kantarjian H, Garcia-Manero G, Borthakur G, O’Brien S, Ravandi F, et al. Failure to attain a significant cytogenetic response by 12 months defines insufficient response in sufferers receiving nilotinib or dasatinib as second or subsequent line remedy for continual myeloid leukemia. Blood. (2008) 112:516–8. doi: 10.1182/blood-2008-02-141580
PubMed Summary | CrossRef Full Textual content | Google Scholar
79. Havrdova E, Hutchinson M, Kurukulasuriya NC, Raghupathi Okay, Sweetser MT, Dawson KT, et al. Oral BG-12 (dimethyl fumarate) for relapsing-remitting a number of sclerosis: a assessment of DEFINE and CONFIRM. Analysis of: Gold R, Kappos L, Arnold D, et al. Placebo-controlled section 3 research of oral BG-12 for relapsing a number of sclerosis. N Engl J Med 2012;367:1098-107. Professional Opin Pharmacother. (2013) 14:2145–56. doi: 10.1517/14656566.2013.826190
PubMed Summary | CrossRef Full Textual content | Google Scholar
80. Vener C, Banzi R, Ambrogi F, Ferrero A, Saglio G, Pravettoni G, et al. First-line imatinib vs second- and third-generation TKIs for chronic-phase CML: a scientific assessment and meta-analysis. Blood Adv. (2020) 4:2723–35. doi: 10.1182/bloodadvances.2019001329
PubMed Summary | CrossRef Full Textual content | Google Scholar
81. Lee SE, Choi SY, Kim SH, Jootar S, Kim HJ, Sohn SK, et al. Comparative analyses of nilotinib versus high-dose imatinib versus sustained standard-dose imatinib in sufferers with continual section continual myeloid leukemia following suboptimal molecular response to first-line imatinib. Leuk Res. (2018) 70:100–5. doi: 10.1016/j.leukres.2018.06.002
PubMed Summary | CrossRef Full Textual content | Google Scholar
82. Cortes JE, Kim DW, Pinilla-Ibarz J, le Coutre P, Paquette R, Chuah C, et al. A section 2 trial of ponatinib in Philadelphia chromosome-positive leukemias. N Engl J Med. (2013) 369:1783–96. doi: 10.1056/NEJMoa1306494
PubMed Summary | CrossRef Full Textual content | Google Scholar
84. Cortes JE, Lomaia E, Turkina A, Moiraghi B, Sutton MU, Pavlovsky C. Interim evaluation (IA) of OPTIC: a dose-ranging research of three ponatinib (PON) beginning doses. J Clin Oncol. (2020) 38:7502. doi: 10.1200/JCO.2020.38.15_suppl.7502
85. Cortes J, Apperley J, Lomaia E, Moiraghi B, Undurraga Sutton M, Pavlovsky C, et al. Ponatinib dose-ranging research in chronic-phase continual myeloid leukemia: a randomized, open-label section 2 medical trial. Blood. (2021) 138:2042–50. doi: 10.1182/blood.2021012082
PubMed Summary | CrossRef Full Textual content | Google Scholar
86. Cortes J, Deininger M, Lomaia E, Moiraghi B, Undurraga Sutton M, Pavlovsky C, et al. Three-year replace from the optic trial: A dose-optimization research of three beginning doses of ponatinib. Blood. (2022) 140:1495–7. doi: 10.1182/blood-2022-157822
87. Devos T, Havelange V, Theunissen Okay, Meers S, Benghiat FS, Gadisseur A, et al. P699: REAL-LIFE OUTCOMES OF PONATINIB TREATMENT IN PATIENTS WITH CHRONIC MYELOID LEUKEMIA (CML) OR PHILADELPHIA CHROMOSOME-POSITIVE ACUTE LYMPHOBLASTIC LEUKEMIA (PH+ALL): 5-YEAR-DATA FROM A BELGIAN REGISTRY. HemaSphere. (2022) 6:594–5. doi: 10.1097/01.HS9.0000845680.44858.4f
88. Breccia M, Olimpieri PP, Celant S, Olimpieri O, Pane F, Iurlo A, et al. Administration of continual myeloid leukaemia sufferers handled with ponatinib in a real-life setting: A retrospective evaluation from the monitoring registries of the Italian Medicines Company (AIFA). Br J Haematol. (2022) 198:965–73. doi: 10.1111/bjh.18359
PubMed Summary | CrossRef Full Textual content | Google Scholar
89. Müller MC, Cervantes F, Hjorth-Hansen H, Janssen JJWM, Milojkovic D, Rea D, et al. Ponatinib in continual myeloid leukemia (CML): Consensus on affected person therapy and administration from a European professional panel. Crit Rev Oncol Hematol. (2017) 120:52–9. doi: 10.1016/j.critrevonc.2017.10.002
PubMed Summary | CrossRef Full Textual content | Google Scholar
90. Saussele S, Haverkamp W, Lang F, Koschmieder S, Kiani A, Jentsch-Ullrich Okay, et al. Ponatinib within the therapy of continual myeloid leukemia and philadelphia chromosome-positive acute leukemia: suggestions of a german professional consensus panel with deal with cardiovascular administration. Acta Haematol. (2020) 143:217–31. doi: 10.1159/000501927
PubMed Summary | CrossRef Full Textual content | Google Scholar
91. Mauro MJ, McGarry LJ, Lustgarden S, Huang H. Predictors of ponatinib remedy length amongst real-world continual section continual myeloid leukemia (CP-CML) sufferers within the US. Blood. (2016) 128:3081–1. doi: 10.1182/blood.V128.22.3081.3081
92. Heiblig M, Rea D, Chrétien ML, Charbonnier A, Rousselot P, Coiteux V, et al. Ponatinib analysis and security in real-life continual myelogenous leukemia sufferers failing greater than two tyrosine kinase inhibitors: the PEARL observational research. Exp Hematol. (2018) 67:41–8. doi: 10.1016/j.exphem.2018.08.006
PubMed Summary | CrossRef Full Textual content | Google Scholar
93. Caocci G, Mulas O, Abruzzese E, Luciano L, Iurlo A, Attolico I, et al. Arterial occlusive occasions in continual myeloid leukemia sufferers handled with ponatinib within the real-life follow are predicted by the Systematic Coronary Danger Analysis (SCORE) chart. Hematol Oncol. (2019) 37:296–302. doi: 10.1002/hon.2606
PubMed Summary | CrossRef Full Textual content | Google Scholar
94. Wylie AA, Schoepfer J, Jahnke W, Cowan-Jacob SW, Bathroom A, Furet P, et al. The allosteric inhibitor ABL001 allows twin focusing on of BCR-ABL1. Nature. (2017) 543:733–7. doi: 10.1038/nature21702
PubMed Summary | CrossRef Full Textual content | Google Scholar
95. Schoepfer J, Jahnke W, Berellini G, Buonamici S, Cotesta S, Cowan-Jacob SW, et al. Discovery of asciminib (ABL001), an allosteric inhibitor of the tyrosine kinase exercise of BCR-ABL1. J Med Chem. (2018) 61:8120–35. doi: 10.1021/acs.jmedchem.8b01040
PubMed Summary | CrossRef Full Textual content | Google Scholar
96. Mauro MJ, Hughes TP, Kim DW, Rea D, Cortes JE, Hochhaus A, et al. Asciminib monotherapy in sufferers with CML-CP with out BCR::ABL1 T315I mutations handled with not less than two prior TKIs: 4-year section 1 security and efficacy outcomes. Leukemia. (2023) 37:1048–59. doi: 10.1038/s41375-023-01860-w
PubMed Summary | CrossRef Full Textual content | Google Scholar
97. Cortes JE, Hughes TP, Mauro MJ, Hochhaus A, Rea D, Goh YT, et al. Asciminib, a first-inclass STAMP inhibitor, supplies sturdy molecular response in sufferers (pts) with continual myeloid leukemia (CML) harboring the T315I mutation: major efficacy and security outcomes from aphase 1 trial. Blood. (2020). doi: 10.1182/blood-2020-139677
98. Hughes T, Mauro M, Kim D, Cortes J, Rea D, Minami H. Asciminib in closely pretreated sufferers with Ph+ CML-CP delicate to TKI remedy. EHA 25 Library. (2020) 37:S170.
99. Hochhaus A, Réa D, Boquimpani C, Minami Y, Cortes JE, Hughes TP, et al. Asciminib vs bosutinib in chronic-phase continual myeloid leukemia beforehand handled with not less than two tyrosine kinase inhibitors: longer-term follow-up of ASCEMBL. Leukemia. (2023) 37:617–26. doi: 10.1038/s41375-023-01829-9
PubMed Summary | CrossRef Full Textual content | Google Scholar
100. Khadadah FM, Cerquozzi S, Olney HJ, Fraga C, Dudebout J, Xenocostas A, et al. Canadian real-world expertise of asciminib therapy in closely pre-treated continual myeloid leukemia (CML) sufferers who failed a number of strains of tyrosine kinase inhibitor (TKI) remedy. Leuk Res. (2023) 133:107374. doi: 10.1016/j.leukres.2023.107374
PubMed Summary | CrossRef Full Textual content | Google Scholar
101. Luna A, Pérez-Lamas L, Boque C, Giraldo P, Xicoy B, Ruiz Nuño C, et al. Actual-life evaluation on security and efficacy of asciminib for ponatinib pretreated sufferers with continual myeloid leukemia. Ann Hematol. (2022) 101:2263–70. doi: 10.1007/s00277-022-04932-6
PubMed Summary | CrossRef Full Textual content | Google Scholar
102. Kockerols CCB, Janssen JJWM, Blijlevens NMA, Klein SK, Van Hussen-Daenen LGM, Van Gorkom GGY, et al. Therapy patterns and medical outcomes of asciminib in a real-world multiresistant continual myeloid leukemia affected person inhabitants. Haematologica. (2022) 108:240–4. doi: 10.3324/haematol.2022.281386
103. Innes AJ, Hayden C, Orovboni V, Rees D, Claudiani S, Fernando F, et al. Actual-world expertise of asciminib: elements related to response. Blood. (2022) 140:6796–7. doi: 10.1182/blood-2022-165501
104. Garcia-Gutiérrez V, Luna A, Alonso-Dominguez JM, Estrada N, Boque C, Xicoy B, et al. Security and efficacy of asciminib therapy in continual myeloid leukemia sufferers in real-life medical follow. Blood Most cancers J. (2021) 11:16. doi: 10.1038/s41408-021-00420-8
PubMed Summary | CrossRef Full Textual content | Google Scholar
105. Yeung DT, Shanmuganathan N, Hughes TP. Asciminib: a brand new therapeutic choice in chronic-phase CML with therapy failure. Blood. (2022) 139:3474–9. doi: 10.1182/blood.2021014689
PubMed Summary | CrossRef Full Textual content | Google Scholar
106. Gandhi V, Plunkett W, Cortes JE. Omacetaxine: a protein translation inhibitor for therapy of continual myelogenous leukemia. Clin Most cancers Res. (2014) 20:1735–40. doi: 10.1158/1078-0432.CCR-13-1283
PubMed Summary | CrossRef Full Textual content | Google Scholar
107. Damlaj M, Lipton JH, Assouline SE. A security analysis of omacetaxine mepesuccinate for the therapy of continual myeloid leukemia. Professional Opin Drug Saf. (2016) 15:1279–86. doi: 10.1080/14740338.2016.1207760
PubMed Summary | CrossRef Full Textual content | Google Scholar
108. Cortes JE, Kantarjian HM, Rea D, Wetzler M, Lipton JH, Akard L, et al. Last evaluation of the efficacy and security of omacetaxine mepesuccinate in sufferers with chronic- or accelerated-phase continual myeloid leukemia: Outcomes with 24 months of follow-up. Most cancers. (2015) 121:1637–44. doi: 10.1002/cncr.29240
PubMed Summary | CrossRef Full Textual content | Google Scholar
109. Jiang Q, Huang X, Chen Z, Niu Q, Males L, Wang H, et al. An up to date security and efficacy outcomes of section 1 research of HQP1351, a novel third era of BCR-ABL tyrosine kinase inhibitor (TKI), in sufferers with TKI resistant continual myeloid leukemia. Blood. (2019) 134:493. doi: 10.1182/blood-2019-124295
PubMed Summary | CrossRef Full Textual content | Google Scholar
110. Jiang Q, Huang X, Chen Z, Niu Q, Shi D, Li Z, et al. Novel BCR-ABL1 tyrosine kinase inhibitor (TKI) HQP1351 (olverembatinib) is efficacious and nicely tolerated in sufferers with T315I-mutated continual myeloid leukemia (CML): outcomes of pivotal (section II) trials. Blood. (2020) 136:50–1. doi: 10.1182/blood-2020-142142
PubMed Summary | CrossRef Full Textual content | Google Scholar
111. Qian J, Shi D, Li Z, Qin Y, Zhao T, Liu B, et al. Up to date security and efficacy outcomes of section 1 research of olverembatinib (HQP1351), a novel third-generation BCR-ABL tyrosine kinase inhibitor (TKI), in sufferers with TKI-resistant continual myeloid leukemia (CML). Blood. (2021) 138:311–1. doi: 10.1182/blood-2021-153065
112. Jiang Q, Li Z, Zhang G, Hu Yu, Li W, Music Y, et al. Olverembatinib (HQP1351) demonstrates efficacy vs. finest obtainable remedy (BAT) in sufferers (pts) with tyrosine kinase inhibitor (TKI)-resistant continual myeloid leukemia chronic-phase (CML-CP) in a registrational randomized section 2 research. Blood. (2023) 142:869, 2023. doi: 10.1182/blood-2023-187740
114. ClinicalTrials.gov. Research to guage tolerability, security, pharmacokinetics and preliminary efficacy of PF-114 for oral administration in adults with Ph+ continual myeloidleukemia, which is immune to the 2nd era Bcr-Abl inhibitors or has T315I mutation within the BCR-ABL gene . Out there on-line at: https://clinicaltrials.gov/ct2/present/NCT02885766 (Accessed Could 2022).
115. Turkina A, Vinogradova O, Lomaia E, Shatokhina E, Shukhov O, ChelyshevaEagles J. PF-114 in sufferers failing prior tyrosine kinase-inhibitor remedy together with BCR::ABL1T315I. Blood. (2021) 138(Complement 1):1482. doi: 10.1182/blood-2021-150120
116. Cortes JE, Kim D, Nicolini FE, Saikia T, Charbonnier A, Apperley JF. Part 1 trial of K0706, a novel oral BCR-ABL1 tyrosine kinase inhibitor (TKI): in sufferers with continual myelogenous leukemia (CML) andPhildelphia optimistic acute lymphoblastic leukemia (Ph+ ALL) failing ≥ 3 prior TKI therapies: preliminary security and efficacy. Blood. (2019) 134:4158. doi: 10.1182/blood-2019-129751
117. Hamilton A, Helgason GV, Schemionek M, Zhang B, Myssina S, Allan EK, et al. Persistent myeloid leukemia stem cells usually are not depending on Bcr-Abl kinase exercise for his or her survival. Blood. (2012) 119:1501–10. doi: 10.1182/blood-2010-12-326843
PubMed Summary | CrossRef Full Textual content | Google Scholar
118. Houshmand M, Simonetti G, Circosta P, Gaidano V, Cignetti A, Martinelli G, et al. Persistent myeloid leukemia stem cells. Leukemia. (2019) 33:1543–56. doi: 10.1038/s41375-019-0490-0
PubMed Summary | CrossRef Full Textual content | Google Scholar
119. Hehlmann R, Voskanyan A, Lauseker M, Pfirrmann M, Kalmanti L, Rinaldetti S, et al. Excessive-risk extra chromosomal abnormalities at low blast counts herald dying by CML. Leukemia. (2020) 34:2074–86. doi: 10.1038/s41375-020-0826-9
PubMed Summary | CrossRef Full Textual content | Google Scholar
120. Passweg JR, Baldomero H, Bader P, Bonini C, Cesaro S, Dreger P, et al. Affect of drug improvement on the usage of stem cell transplantation: a report by the European Society for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant. (2017) 52:191–6. doi: 10.1038/bmt.2016.258
PubMed Summary | CrossRef Full Textual content | Google Scholar
121. Passweg JR, Baldomero H, Bader P, Bonini C, Duarte RF, Dufour C, et al. Use of haploidentical stem cell transplantation continues to extend: the 2015 European Society for Blood and Marrow Transplant exercise survey report. Bone Marrow Transplant. (2017) 52:811–7. doi: 10.1038/bmt.2017.34
PubMed Summary | CrossRef Full Textual content | Google Scholar
122. Lübking A, Dreimane A, Sandin F, Isaksson C, Märkevärn B, Brune M, et al. Allogeneic stem cell transplantation for continual myeloid leukemia within the TKI period: population-based knowledge from the Swedish CML registry. Bone Marrow Transplant. (2019) 54:1764–74. doi: 10.1038/s41409-019-0513-5
PubMed Summary | CrossRef Full Textual content | Google Scholar
123. Arora M, Weisdorf DJ, Spellman SR, Haagenson MD, Klein JP, Hurley CK, et al. HLA-identical sibling in contrast with 8/8 matched and mismatched unrelated donor bone marrow transplant for continual section continual myeloid leukemia. J Clin Oncol. (2009) 27:1644–52. doi: 10.1200/JCO.2008.18.7740
PubMed Summary | CrossRef Full Textual content | Google Scholar
124. Radich JP, Gooley T, Bensinger W, Chauncey T, Clift R, Flowers M, et al. HLA-matched associated hematopoietic cell transplantation for chronic-phase CML utilizing a focused busulfan and cyclophosphamide preparative routine. Blood. (2003) 102:31–5. doi: 10.1182/blood-2002-08-2619
PubMed Summary | CrossRef Full Textual content | Google Scholar
125. Gratwohl A, Pfirrmann M, Zander A, Kröger N, Beelen D, Novotny J, et al. Lengthy-term consequence of sufferers with newly identified continual myeloid leukemia: a randomized comparability of stem cell transplantation with drug therapy. Leukemia. (2016) 30:562–9. doi: 10.1038/leu.2015.281
PubMed Summary | CrossRef Full Textual content | Google Scholar
126. Bacher U, Klyuchnikov E, Zabelina T, Ottinger H, Beelen DW, Schrezenmeier H, et al. The altering scene of allogeneic stem cell transplantation for continual myeloid leukemia–a report from the German Registry overlaying the interval from 1998 to 2004. Ann Hematol. (2009) 88:1237–47. doi: 10.1007/s00277-009-0737-3
PubMed Summary | CrossRef Full Textual content | Google Scholar
127. Ohashi Okay, Nagamura-Inoue T, Nagamura F, Tojo A, Miyamura Okay, Mori T, et al. Impact of graft sources on allogeneic hematopoietic stem cell transplantation consequence in adults with continual myeloid leukemia within the period of tyrosine kinase inhibitors: a Japanese Society of Hematopoietic Cell Transplantation retrospective evaluation. Int J Hematol. (2014) 100:296–306. doi: 10.1007/s12185-014-1632-9
PubMed Summary | CrossRef Full Textual content | Google Scholar
128. Chaudhury S, Sparapani R, Hu ZH, Nishihori T, Abdel-Azim H, Malone A, et al. Outcomes of allogeneic hematopoietic cell transplantation in youngsters and younger adults with continual myeloid leukemia: A CIBMTR cohort evaluation. Biol Blood Marrow Transplant. (2016) 22:1056–64. doi: 10.1016/j.bbmt.2016.02.015
PubMed Summary | CrossRef Full Textual content | Google Scholar
129. Lee SE, Choi SY, Kim SH, Jang EJ, Bang JH, Byeun JY, et al. Prognostic elements for outcomes of allogeneic stem cell transplantation in continual section continual myeloid leukemia within the period of tyrosine kinase inhibitors. Hematology. (2014) 19:63–72. doi: 10.1179/1607845413Y.0000000100
PubMed Summary | CrossRef Full Textual content | Google Scholar
130. Koenecke C, Heim D, van Biezen A, Heuser M, Aljurf M, Kyrcz-Krzemien S, et al. Consequence of sufferers with continual myeloid leukemia and a low-risk rating: allogeneic hematopoietic stem cell transplantation within the period of focused remedy. A report from the EBMT Persistent Malignancies Working Get together. Bone Marrow Transplant. (2016) 51:1259–61. doi: 10.1038/bmt.2016.97
PubMed Summary | CrossRef Full Textual content | Google Scholar
131. Saussele S, Lauseker M, Gratwohl A, Beelen DW, Bunjes D, Schwerdtfeger R, et al. Allogeneic hematopoietic stem cell transplantation (allo SCT) for continual myeloid leukemia within the imatinib period: analysis of its affect inside a subgroup of the randomized German CML Research IV. Blood. (2010) 115:1880–5. doi: 10.1182/blood-2009-08-237115
PubMed Summary | CrossRef Full Textual content | Google Scholar
132. Soverini S, Colarossi S, Gnani A, Castagnetti F, Rosti G, Bosi C, et al. Resistance to dasatinib in Philadelphia-positive leukemia sufferers and the presence or the choice of mutations at residues 315 and 317 within the BCR-ABL kinase area. Haematologica. (2007) 92:401–4. doi: 10.3324/haematol.10822
PubMed Summary | CrossRef Full Textual content | Google Scholar
133. Oyekunle A, Zander AR, Binder M, Ayuk F, Zabelina T, Christopeit M, et al. Consequence of allogeneic SCT in sufferers with continual myeloid leukemia within the period of tyrosine kinase inhibitor remedy. Ann Hematol. (2013) 92:487–96. doi: 10.1007/s00277-012-1650-8
PubMed Summary | CrossRef Full Textual content | Google Scholar
134. Piekarska A, Gil L, Prejzner W, Wiśniewski P, Leszczyńska A, Gniot M, et al. Pretransplantation use of the second-generation tyrosine kinase inhibitors has no detrimental affect on the HCT consequence. Ann Hematol. (2015) 94:1891–7. doi: 10.1007/s00277-015-2457-1
PubMed Summary | CrossRef Full Textual content | Google Scholar
135. Goldman JM, Majhail NS, Klein JP, Wang Z, Sobocinski KA, Arora M, et al. Relapse and late mortality in 5-year survivors of myeloablative allogeneic hematopoietic cell transplantation for continual myeloid leukemia in first continual section. J Clin Oncol. (2010) 28:1888–95. doi: 10.1200/JCO.2009.26.7757
PubMed Summary | CrossRef Full Textual content | Google Scholar
136. Kondo T, Nagamura-Inoue T, Tojo A, Nagamura F, Uchida N, Nakamae H, et al. Scientific affect of pretransplant use of a number of tyrosine kinase inhibitors on the end result of allogeneic hematopoietic stem cell transplantation for continual myelogenous leukemia. Am J Hematol. (2017) 92:902–8. doi: 10.1002/ajh.24793
PubMed Summary | CrossRef Full Textual content | Google Scholar
137. Rezvani Okay, Kanfer EJ, Marin D, Gabriel I, Rahemtulla A, Taylor A, et al. EBMT threat rating predicts consequence of allogeneic hematopoietic stem cell transplantation in sufferers who’ve failed a earlier transplantation process. Biol Blood Marrow Transplant. (2012) 18:235–40. doi: 10.1016/j.bbmt.2011.06.010
PubMed Summary | CrossRef Full Textual content | Google Scholar
138. Chhabra S, Ahn KW, Hu ZH, Jain S, Assal A, Cerny J, et al. Myeloablative vs reduced-intensity conditioning allogeneic hematopoietic cell transplantation for continual myeloid leukemia. Blood Adv. (2018) 2:2922–36. doi: 10.1182/bloodadvances.2018024844
PubMed Summary | CrossRef Full Textual content | Google Scholar
{kind=link}