
1 Introduction
The incidence and mortality of colorectal most cancers (CRC) have been drastically diminished by large-scale screening for lesions in colon and rectum amongst average-risk populations (1). Many international locations and areas have offered organized CRC screening for middle-aged and aged populations as native or nationwide public well being service applications (2). The triage screening technique, principally colonoscopy referral for people with optimistic fecal immunochemical check (FIT) outcomes, was broadly adopted within the applications (3, 4). Nevertheless, FIT is just not delicate to non-bleeding lesions. Subsequently, a number of threat scoring programs have been developed and used combinatorically with FIT to establish high-risk people for subsequent colonoscopy, significantly in Asia-Pacific international locations with a low incidence of the most cancers (5).
In China, the questionnaire-based threat evaluation (RA) and two-sample qualitative FIT has been parallel used to detect CRC since 2005 (6). The parallel exams have been proved cost-effective in Chinese language populations (7), and have been really helpful as preliminary exams for CRC screening applications in China. To date, nonetheless, the general public well being service applications have been offered solely in Shanghai (8), Guangzhou (9), Tianjin (10), Hangzhou (11), and different city areas, together with the population-based Most cancers Screening Program in City China (CanSPUC) program that lined 22 cities in 16 provinces and used a threat scoring system incorporating earlier fecal occult blood check outcomes (12). The utility of the RA instruments, nonetheless, has been constantly noticed to end in suboptimal adherence to colonoscopy, which drastically jeopardized the effectivity of CRC screening (11–14). In our earlier research, we discovered that the colonoscopy adherence was lower than 40%, and positively associated with the specificity of preliminary screening exams (14, 15).
With the event of biotechnology, plenty of novel exams have been developed lately, during which colon capsule endoscopy, computed tomographic colonography, and molecular biomarkers in stool or blood at DNA, RNA and protein ranges are promising in CRC screening (16, 17). Of the novel biomarkers, multi-target stool DNA check (mt-sDNA) and methylated SEPT9 DNA plasma assay (mSEPT9) have been really helpful as complementary exams for FIT within the 2016 USPSTF guideline (18). These rising applied sciences present a number of selections of screening exams, which can break the bottlenecks of the present screening modalities and promote optimization and diversification of screening methods.
To higher perceive the benefits and downsides of the currently-used screening exams for CRC in China, and the potential purposes of the novel exams in large-scale CRC screening practices, we carried out a qualitative examine based mostly on grounded idea. The grounded idea focuses on revealing the method of a phenomenon and the various views concerning the phenomenon, thereby creating an explanatory idea for this phenomenon (19). The speculation emphasizes the theoretical sampling, fixed comparability of information, and theoretical saturation. The simultaneous knowledge assortment and evaluation permit theoretical sampling of interviewees who can present info to develop a idea and eventually attain theoretical saturation (20).
The grounded idea gives an excellent qualitative methodological framework to discover viewpoints of specialists on the scenario of CRC screening and the utility of novel screening exams in China, which can assist to optimize and replace the screening tips, facilitate identification of high-risk people for colonoscopy, and enhance effectivity of CRC screening applications in China.
2 Strategies
2.1 Examine design
On this qualitative examine using an exploring analysis expertise of grounded idea (19), a semi-structured open-ended particular person interview was carried out in China from October to November of 2020. The examine was reported based on the Consolidated Standards for Reporting Qualitative Analysis (COREQ) reporting guideline (21).
This examine was authorised by the Ethics Committee of Fudan College Faculty of Public Well being (IRB00002408 & FWA00002399) (Registration quantity: 2019-TYSQ-03-29). Previous to the graduation of every interview, every participant was knowledgeable of the aim of the examine and the voluntary, nameless, and confidential nature of the interview utilizing an info sheet. All contributors have been additionally knowledgeable of that the lengthy interview interval would trigger minimal discomfort, and their withdrawal from the examine could be permitted with none opposed outcomes. The contributors have been required to signal an knowledgeable consent kind earlier than collaborating. The authors declare that the examine was carried out in accordance with the Declaration of Helsinki for analysis involving human topics (22).
2.2 Examine contributors
To make sure satisfactory representativeness and variety of the viewpoints, the examine contributors have been chosen from totally different well being sections of presidency, analysis institutes, facilities for illness prevention and management (CDC), hospitals, and group healthcare facilities in China utilizing a purposive sampling methodology. Their career, place, expertise, and information in CRC screening have been additionally thought of to make sure the complete protection of the service supply (i.e., policy-making, administration, supervision, group, implementation, follow-up, analysis and remedy, and analysis). The potential specialists have been invited to take part the interview by phone-call or sending an e mail, after which contributors have been scheduled for an interview at a handy time. A complete of 15 contributors have been interviewed. The contributors’ traits are introduced in Desk 1.
2.3 Knowledge assortment
In-depth interviews have been carried out utilizing an interview define conceptualized and developed based mostly on the Consolidated Framework for Implementation Analysis (CFIR) (23), which has been broadly utilized in well being service analysis (24). The 5 main domains of CFIR-intervention traits, outer setting, internal setting, traits of people, and implementation course of—have been used to virtually information the analysis of boundaries and facilitators of interventions (23), and due to this fact could also be appropriate for the evaluation of the CRC screening.
Based mostly on systematic iterations of scientific literature evaluations and cautious choice and rephrasing of the gadgets, we developed an interview define together with 12 most fitted probing questions in regards to the present CRC screening protocol, boundaries and facilitators for screening effectiveness, current issues and potential optimization of screening protocol, and future prospects of CRC screening applications (Determine 1). Additional dialogue was carried out together with the probing questions. We additionally collected reported sensitivity, specificity and value of currently-used preliminary screening exams via complete literature evaluations and consults with associated specialists. The data summarized in Desk 2 was offered to the contributors as a reference on the interview, which was supplemented on the similar time by the specialists interviewed. The protocol of the interview was pilot-tested with one skilled (ID11) to find out the readability, reliability, and convergent validity of the questions. Because the pilot interview simply indicated minor adjustment of the merchandise order and language expression, however didn’t reveal any want for main modifications to the interview schedule, the outcomes of the pilot check have been included on this evaluation.
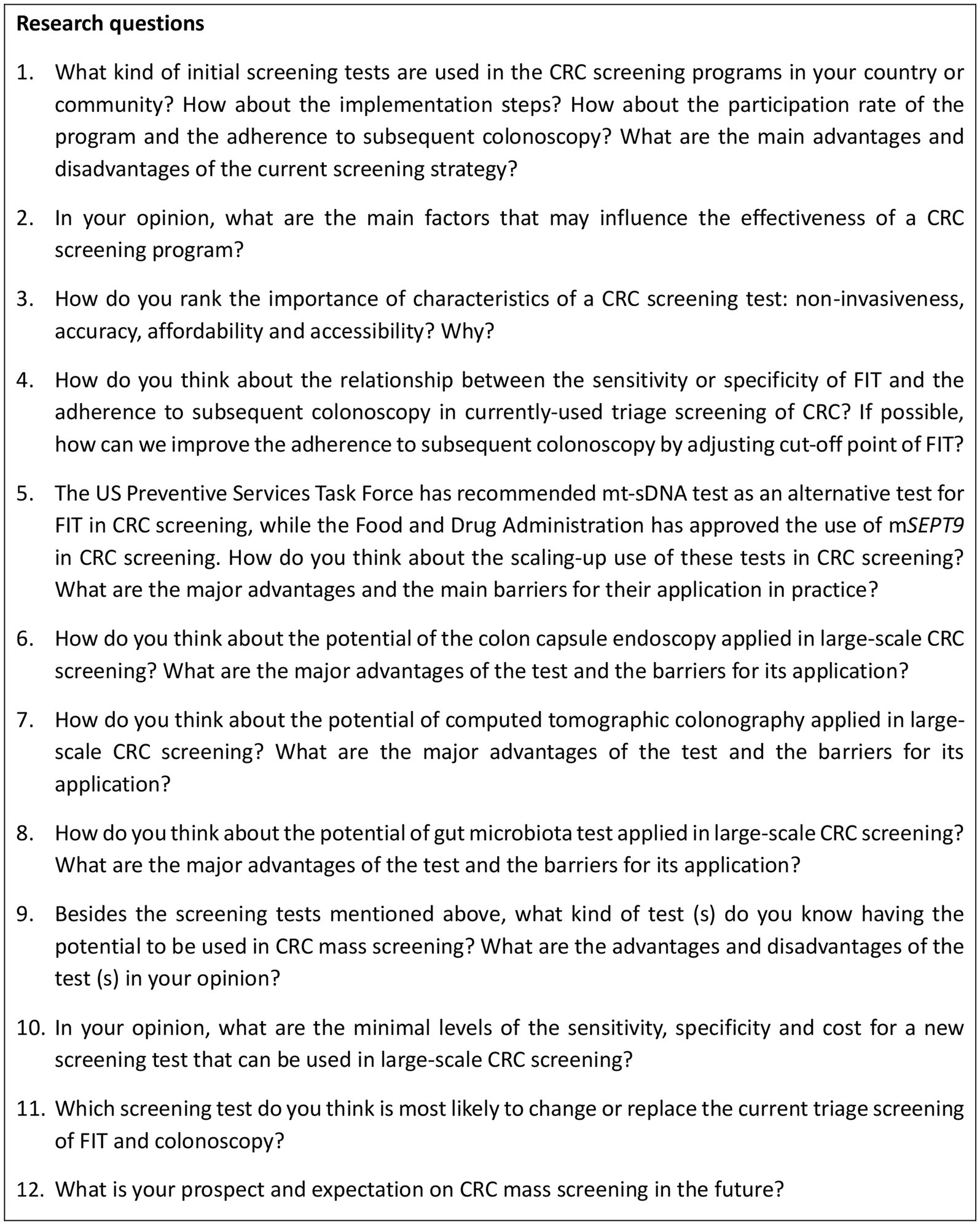
Determine 1. Interview information to discover viewpoints of specialists on CRC screening. CRC: colorectal most cancers; FIT: fecal immunochemical check; mSEPT9: methylated SEPT DNA plasma assay; mt-sDNA: multi-target stool DNA check.
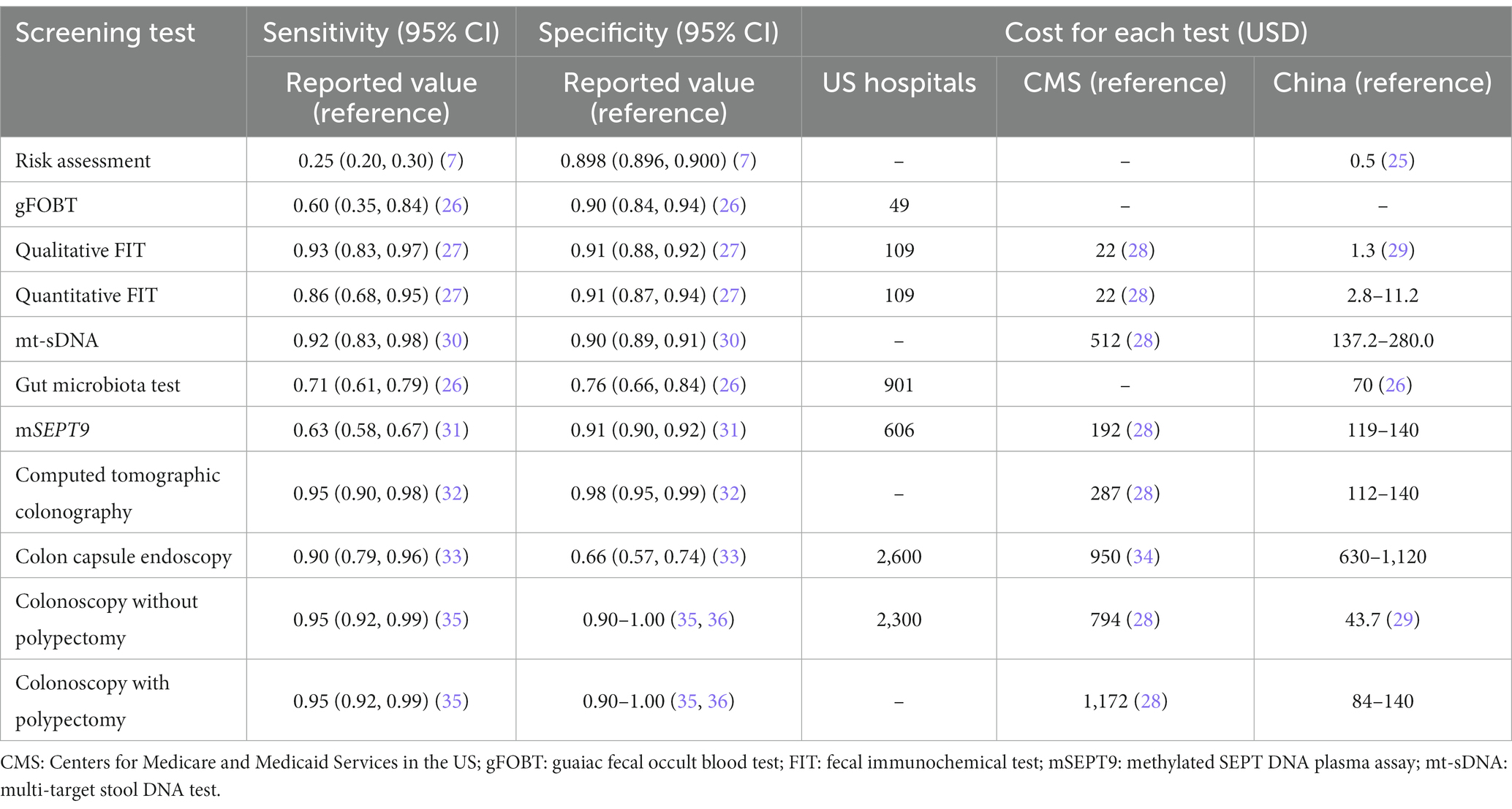
Desk 2. Earlier reported sensitivity, specificity, and value of every screening check for colorectal most cancers.
The face-to-face interviews have been carried out with 5 specialists at their workplaces or a non-public room the place nobody may observe or overhear the discussions. On-line interviews have been additionally carried out for 10 specialists utilizing Zoom, Tencent, or WeChat. The primary researcher (W.M.W.) moderated the interviews utilizing follow-up prompts for readability, and requested for added info when wanted. The second researcher (S.S.T.) took area notes to evaluate gestures, facial expressions and different non-verbal communications of the contributors, and offered technical assist throughout the interviews. The interviews have been audio-recorded utilizing a smartphone. The interviews lasted for 40 min roughly, which ranged from 30 to 60 min. Following rigorous standardized method for qualitative analysis, the information assortment was terminated when knowledge saturation was achieved.
After the interviews, a self-administered questionnaire was used to gather demographic traits of specialists, together with age, intercourse, instructional stage, occupation, skilled title, period of working within the space of CRC screening, and their roles within the space of CRC screening.
2.4 Knowledge evaluation
Audio recordings of the interviews have been transcribed verbatim utilizing iflyrec software program. The transcripts have been double-checked and transferred to MAXQDA 2020 software program by the researchers. An iterative knowledge assortment and evaluation have been employed utilizing a continuing comparability method to construct ideas and classes based on the grounded idea method, which gives a radical procedure-oriented methodology for coding, together with open, axial, and selective coding phases.
Open coding includes breaking down, analyzing, evaluating, conceptualizing, and classifying knowledge, via which the central ideas and classes have been created. Axial coding additional labeled, condensed, and refined the classes to develop subcategories associated to every fundamental class. Selective coding, the third part, additional abstracted and summarized the principle classes to kind the core classes, and eventually construct a grounded theoretical mannequin overlaying all of the collected knowledge (37). A theoretical saturation check was carried out throughout and after the method of coding till no further points or insights have been recognized (17). On this interview, no new idea or class was discovered when the transcripts of the eleventh respondent have been coded. Extra 4 specialists have been interviewed to substantiate the theoretical saturation. To extend the reliability of our findings, two researchers coded all of the transcripts independently. A 3rd researcher checked the unique knowledge, coding, extracted ideas and classes, and in contrast and mentioned any controversy to achieve a consensus.
3 Outcomes
Greater than 600 min of audio recordings have been collected and transcribed verbatim, from which the ideas associated to the goals of this examine have been extracted. After which 83 preliminary classes have been derived from the ideas within the open coding part. Then 37 subcategories and 10 fundamental classes have been summarized from the preliminary classes via axial coding. Within the selective coding, 4 core classes have been recognized, together with present modality for CRC screening (C1), elements influencing screening effectiveness (C2), optimization of CRC screening modality (C3), and prospects for growth (C4) (Desk 3).
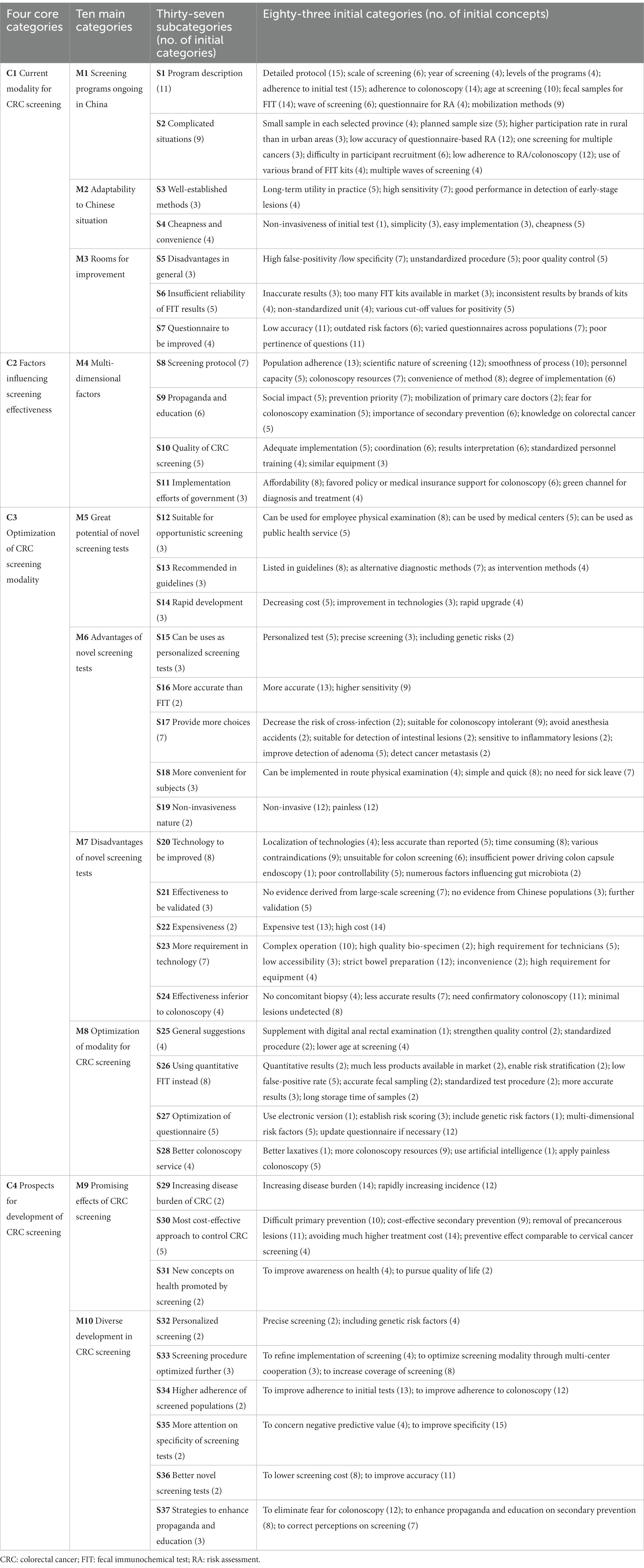
Desk 3. Classes extracted by open coding, axial coding and selective coding.
3.1 Classes and sub-categories
3.1.1 C1: present CRC screening modality in China
The nationwide guideline of China for CRC screening really helpful parallel use of RA and two-sample qualitative FIT as preliminary exams, adopted by a colonoscopy follow-up (6). This triage screening technique is being carried out as a significant public well being service in Shanghai (8), Guangzhou (9), and Hangzhou (11). Within the CanSPUC program initiated in 2012 in mainland China, a threat scoring system was used as an preliminary check (12). In Taiwan and Hong Kong, one-sample quantitative FIT was used to establish high-risk people for subsequent colonoscopy (38, 39). Virtually all specialists expressed their issues on the excessive false-positive charges of the preliminary exams, and proposed a number of potential contributors to the opposed scenario.
First, varied qualitative FIT merchandise have been utilized in screening applications as an preliminary check. Qualitative FIT is often utilized in China attributable to its comfort and cheapness. Nevertheless, greater than 10 manufacturers of qualitative FIT kits produced by totally different producers can be found in China, however with low consistency in check outcomes. For the quantitative FIT, quite the opposite, just one product with a model of OC-MICRO is obtainable dominantly in China.
“Quantitative FIT is broadly utilized in developed international locations or areas, whereas qualitative FIT is extra commonly-used in China. The low consistency of the outcomes examined by totally different manufacturers of qualitative FIT kits have change into a giant downside within the follow of CRC screening.” (Male, researcher, ID14)
“The outcomes of qualitative exams should not constant for FIT kits produced by totally different producers. Nevertheless, totally different FIT kits have been used throughout screening applications; even in a CRC screening program, the FIT kits could change 12 months by 12 months.” (Feminine, CDC workers, ID7)
Second, the really helpful RA instruments haven’t been up to date. The danger elements of CRC could have modified together with the social growth and dietary transition in China. Nevertheless, the RA instruments haven’t been up to date based mostly on newly-established threat predictive fashions or threat scoring programs.
“The questionnaire at present used was derived from a number of case-control research carried out in Jiashan County, Zhejiang Province, a number of a long time in the past, and was simply simplified in a large-scale nationwide most cancers screening program lately. Clearly, the questionnaire is outdated. We’ve steered to replace the questionnaire throughout the previous years.” (Male, main care supplier, ID1)
“Usually, folks have been much less more likely to attend follow-up colonoscopy in the event that they have been recognized as high-risk people by questionnaire-based RA solely. The danger stratification based mostly on the outcomes of the questionnaire was not convincing for our topics.” (Feminine, main care supplier, ID9)
Lastly, varied misconducts could occur in every a part of the entire process of screening, which can have led to inaccurate check outcomes.
“Most topics would report having constipation or diarrhea even when they’d the signs sometimes, if docs didn’t clarify associated definitions very clearly throughout the survey. This is able to result in low high quality of the collected knowledge and incorrect threat stratifications” (Male, gastroenterologist, ID2)
“The contributors have been requested to gather fecal samples by themselves. Nevertheless, it’s tough for them to gather applicable quantity of stool samples. Some contributors even added water into the tubes …. The operation was positively unstandardized and incorrect.” (Feminine, researcher, ID12)
3.1.2 C2: elements influencing screening effectiveness
The specialists’ opinions on boundaries and facilitators for effectiveness of CRC screening have been additionally collected. Particularly, the specialists have been extremely involved concerning the inhabitants adherence, rationality, and affordability of CRC screening exams. As introduced in Desk 4, the accuracy and the affordability ranked the primary and the second of the 4 vital traits of screening exams (accuracy, affordability, accessibility and non-invasiveness) based on the viewpoints of the specialists.
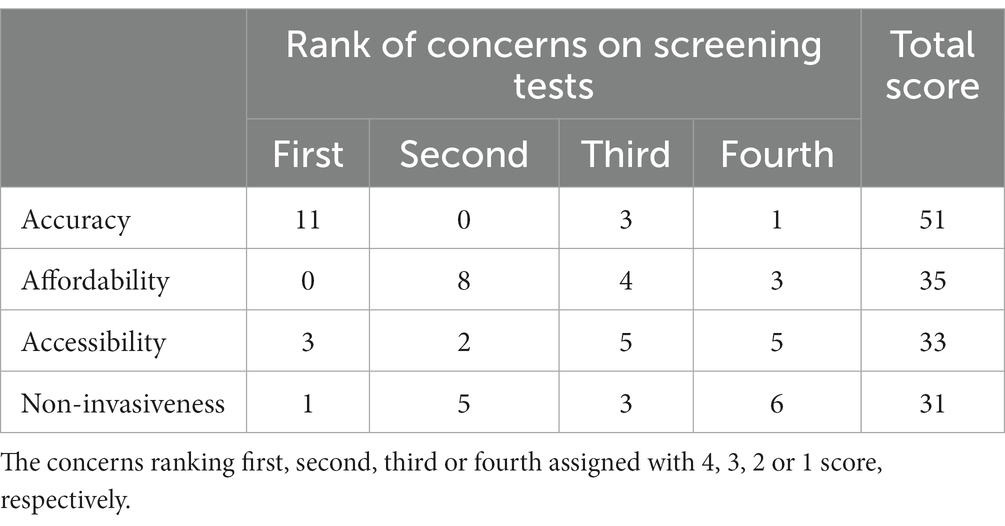
Desk 4. The issues of specialists on the traits of screening exams for colorectal most cancers.
As proven in Determine 2, a complete of 13 specialists believed that adherence to subsequent colonoscopy was associated to the accuracy of FIT. Amongst them, 7 specialists proposed that the specificity of FIT was extra vital than different indices of accuracy, 6 specialists thought that prime false-positive charge of FIT could have led to the mistrust of screening leads to screened populations, 4 specialists believed that larger accuracy of preliminary check outcomes strengthen confidence for attending the next colonoscopy examination, and 4 specialists talked about the potential group impact in attending subsequent colonoscopy.
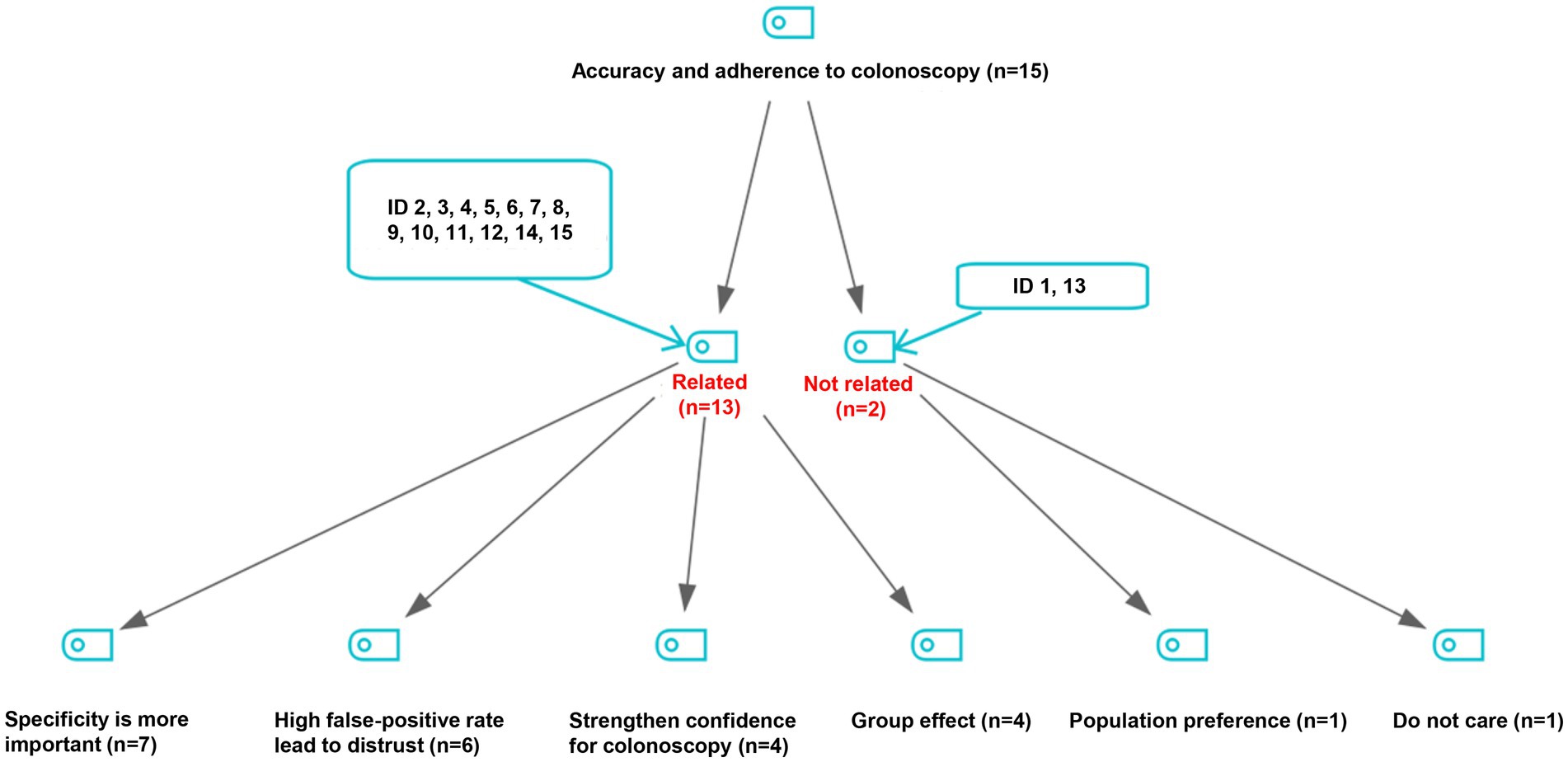
Determine 2. Viewpoints on the connection of accuracy of preliminary screening exams with adherence to follow-up colonoscopy.
“The CRC screening was carried out spherical by spherical, and a number of waves of screening have been carried out in lots of locations. Sadly, a vicious circle was noticed attributable to excessive false-positive charge of the preliminary screening check: a excessive false-positive charge of an preliminary check could lower the adherence to subsequent colonoscopy, and additional impedes the sustainability of CRC screening applications.” (Feminine, researcher, ID6)
“For instance, a topic recognized as high-risk by preliminary screening exams could really feel tricked, if he/she was not discovered any lesions in subsequent colonoscopy examination. Then he/she would categorical his/her mistrust of the preliminary check outcomes to his/her friends, which can additional lower adherence to colonoscopy in the neighborhood” (Feminine, CDC workers, ID11)
3.1.3 C3: optimization of CRC screening modality
Regardless of the issues current in present screening modality, the specialists believed that the modality might be optimized via bettering course of administration (S25), making use of quantitative FIT (S26), updating RA instruments (S27), and offering higher colonoscopy service (S28) (Desk 3). Notably, the specialists steered to reinforce the pertinence of things for RA by excluding outdated questions like persistent appendicitis or appendectomy, persistent cholecystitis or cholecystectomy, persistent constipation and persistent diarrhea, and including a number of vital threat elements into the system, corresponding to physique mass index (BMI), bodily exercise, aspirin use, weight loss program and smoking.
“We now use the questionnaire-based RA derived from the surveys in Jiashan County and Haining Metropolis of Zhejiang Province within the Nineteen Nineties. The RA instrument could also be outdated, and didn’t precisely replicate the danger exposures these days. The danger elements of CRC have been altering over time, and BMI, bodily actions and smoking must be included within the questionnaire now.” (Feminine, CDC workers, ID7)
The specialists additionally proposed to make use of 1-sample FIT as an alternative of 2-sample exams, or apply quantitative FIT as an alternative of inaccurate qualitative exams. Concerning the affordability, most specialists thought that the price of 20 CNY per quantitative check is appropriate in China.
“For the FIT, I like to recommend 1-sample FIT as an alternative of 2-sample exams based on the outcomes of our screening program, and as most international locations did.” (Male, researcher, ID14)
“Lately, I heard that an company of OC-MICRO (a model of FIT) in Hangzhou offered the associated fee per capita of 20 CNY. The federal government of Zhejiang Province has launched a program for early detection of most cancers, and intends to make use of quantitative FIT, however I do not know whether or not they’re utilizing it this 12 months.” (Male, main care supplier, ID1)
“In my view, there isn’t any downside with CRC screening exams and the bottom line is to totally understand the effectiveness of every half in the entire screening course of. Nevertheless, a giant hole existed between the noticed and the anticipated effectiveness of a sure screening program. I feel crucial is to totally understand the anticipated effectiveness of every check in CRC screening follow.” (Feminine, researcher, ID12)
3.1.4 C4: prospects for growth of CRC screening
The a lot larger prices of the novel screening exams for CRC than RA, FIT and even colonoscopy would restrict the widespread use of those novel exams in China, a rustic with an enormous inhabitants and inadequate medical assets. As proven in Desk 2, the price of colonoscopy is way decrease in China (44 USD) than in the USA (2,300 USD), which devalue and limit the applying of the accessible novel CRC screening exams in China.
On this examine, 9 specialists (ID 1, 4, 5, 7, 8, 9, 12, 13, 14) believed that not one of the accessible novel CRC screening exams is nice sufficient to interchange the triage screening strategies which can be at present used. Nevertheless, they acknowledged that a number of novel exams can be utilized as a substitute screening methodology, and have nice potential in opportunistic screening. 5 specialists (ID 2, 3, 10, 11, 15) believed that mt-sDNA check is probably the most promising novel methodology for CRC screening within the close to future.
“As a result of comparatively excessive price, the novel exams could also be used as the choice strategies in customized service. Nevertheless, the federal government can merely present primary public well being providers however not the customized ones. We will present the residents with totally different alternate options, however it’s not economically sensible for presidency to cowl all of the bills.” (Male, well being official, ID5)
“The mt-sDNA check can assist to enhance sensitivity and enhance participation charge of screening … you’ll be able to alter threshold of mt-sDNA check for extra focused screening, which I feel is an efficient factor. The mt-sDNA check contains quantitative molecular assays for hemoglobin, genetic mutations, methylation, and so forth. I feel it’s of nice significance for CRC screening.” (Male, gastroenterologist, ID3)
3.2 Mannequin building
Based mostly on the subcategories, fundamental classes and core classes recognized in Desk 3, the important points in CRC screening in China will be summarized right into a grounded theoretical mannequin in Determine 3. Over the previous a long time, the triage screening modality utilized in CRC screening applications (M1) has been discovered fairly appropriate for China and broadly adopted within the nation attributable to its cheapness and comfort (M2). Nevertheless, there are a number of challenges (M3), significantly the suboptimal adherence to colonoscopy that has drastically lowered the effectiveness of screening applications. Elements concerning well being propaganda and schooling, high quality management and authorities may additionally affect the effectiveness of screening applications (M4). Thankfully, the CRC screening applications will be improved by making use of novel screening exams (M5) or optimizing present screening modality (M8). Regardless of the benefits and good prospects of the novel screening exams (M6), their excessive prices and excessive technical requirement have restricted their utility in large-scale screening applications (M7). Subsequently, optimization of present screening modality (M8) is very anticipated, which will be achieved by utilizing extra correct threat stratification, making use of quantitative FIT, and offering higher colonoscopy service. Within the opinions of the specialists interviewed, contemplating the widely acknowledged effectiveness of CRC screening (M9), the various growth in CRC screening is very anticipated, together with customized screening, optimized screening process, larger inhabitants adherence, larger specificity of preliminary exams, use of novel screening exams, and improved well being schooling (M10).
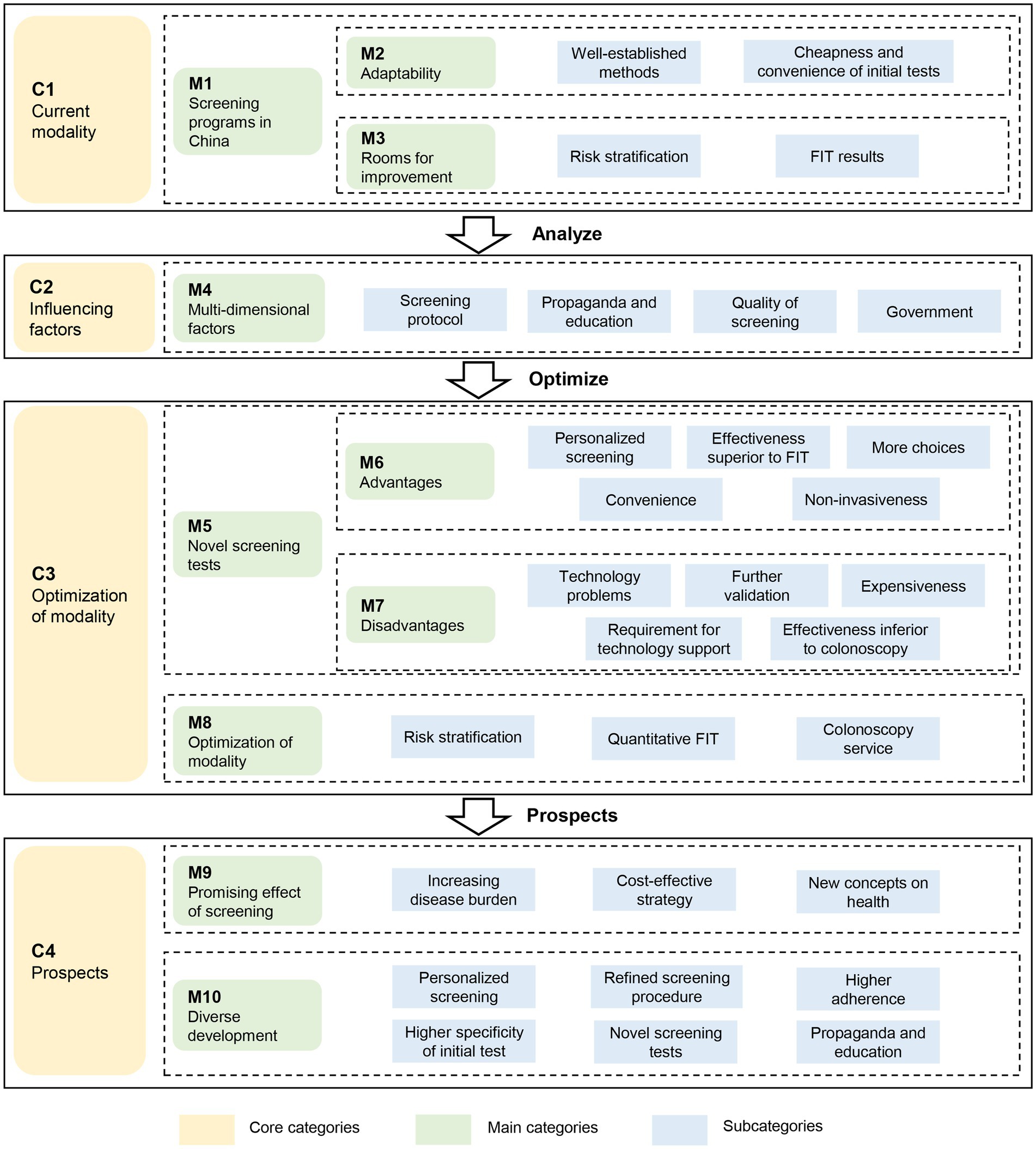
Determine 3. The grounded theory-based framework to judge the screening methods for colorectal most cancers. FIT: fecal immunochemical check.
4 Dialogue
On this examine, we explored the viewpoints of 15 specialists concerning the CRC screening modality in China via semi-structured interviews. Usually, the specialists responded positively to the triage screening modality adopted in China, but in addition expressed issues on the low adherence to colonoscopy amongst high-risk topics who have been recognized by preliminary screening exams. The specialists steered to optimize the preliminary screening check by utilizing quantitative FIT as an alternative of the qualitative one, and by updating the RA instruments currently-used in China. For the rising screening applied sciences, the specialists proposed to make use of the novel exams as supplementary strategies to the triage screening modalities. The opinions could assist to optimize the currently-used screening modality for CRC, enhance adherence to follow-up colonoscopy, and absolutely obtain the effectiveness of screening applications in China.
The effectiveness of CRC screening applications is dependent upon the accuracy of screening exams and the adherence of screened populations (40). A low adherence to colonoscopy was constantly noticed amongst high-risk topics recognized by preliminary exams in China (8, 12). On this examine, most specialists believed that adherence to colonoscopy was influenced by the accuracy of FIT, probably the most generally used preliminary check in triage screening for CRC globally. In our earlier research, we discovered that adherence to colonoscopy was positively related to specificity and optimistic predictive worth of preliminary screening exams (14, 15), which was consistent with the findings in different populations (41, 42). Subsequently, the excessive false-positive charge of preliminary exams in China was the widespread concern of the specialists on this examine.
To launch the priority, the specialists proposed two approaches to lower false-positive charge of the preliminary exams, which can assist to enhance the adherence to subsequent colonoscopy in China. First, the skilled really helpful to make use of quantitative FIT as an alternative of the qualitative one. The quantitative FITs outperform the qualitative ones not solely attributable to its larger accuracy, but in addition for its versatile cut-off values (43). Nevertheless, quantitative FIT stays to be developed for the large-scale screening practices in China attributable to its comparatively larger price. Furthermore, the sensitivity and specificity of one-sample qualitative FIT was discovered much like these of multiple-sample exams, whatever the model of FIT merchandise (27). Evidently, one-sample FIT must be adopted in China to simplify the screening process, enhance participation charge, and scale back calls for for colonoscopy (44). Second, the specialists proposed to replace the RA instruments. The currently-used RA instrument didn’t embrace age, intercourse, smoking, consuming, BMI, weight loss program, bodily exercise, analysis of diabetes, use of non-steroidal anti-inflammatory medication or aspirin (8, 11, 12), the widespread threat elements of CRC included in different threat scoring programs (45, 46) and really helpful within the up to date Chinese language guideline for CRC screening (32). It was additionally discovered that a number of elements for RA will be faraway from questionnaire with none further missed CRC instances (47). Thus, the RA instruments is urgently wanted to be up to date utilizing population-and period-specific threat elements of CRC for higher accuracy and applicability.
Lately, many novel CRC screening exams have been developed to interchange or scale back invasive examination like colonoscopy. Nevertheless, the inconsistent efficiency of those exams in populations has restricted their widespread purposes (32, 48). In spite of everything, the accuracy is crucial characteristic of a screening check. On this examine, we discovered that the specialists ranked affordability the second most vital characteristic of screening exams, significantly for large-scale screening applications. Most novel screening exams are costly and typically require further technical assist. For instance, about 512 USD is required for one mt-sDNA check, a lot decrease than 1,172 USD for a colonoscopy within the US. Subsequently, mt-sDNA check is really helpful within the guideline in all probability for the consideration of cost-effectiveness. In China, nonetheless, solely 44 USD is required for a colonoscopy examination, a lot decrease than the prices in western international locations (28, 29). Subsequently, it’s cheaper to use colonoscopy in China, the reference check in CRC screening. To date, the novel exams are steered for use in opportunistic screening in bodily examination establishments or hospitals.
This examine has a number of limitations. First, we didn’t interview the contributors of CRC screening applications, who could present further opinions on the CRC screening applications in China. Nevertheless, as this qualitative interview examine was designed from the angle of service suppliers, and the opinions of the specialists have been derived from their expertise and interactions with the screened topics, our outcomes have nice values for evidence-based coverage making. Second, the interview was carried out within the Chinese language setting with country-specific coverage, sensible situation, and educational points, which inevitably brings the query of whether or not the mannequin was common and relevant in different international locations. Lastly, the conclusions of this examine have been made via a theoretical dialogue, not based mostly on a real-world screening knowledge evaluation. Nevertheless, we summarized the sensitivity, specificity and value of every currently-used preliminary screening exams via complete literature evaluations, and offered the data to our topics on the interview, which can have made the dialogue evidence-based.
5 Conclusion
Within the opinions of specialists in China, the triage screening modality, if improved, stays the optimum selection for Chinese language populations. To make use of quantitative FIT or replace RA instruments could assist to establish high-risk people extra precisely, enhance adherence to subsequent colonoscopy, and thus absolutely obtain the effectiveness of screening. The rising novel applied sciences have nice potentials in opportunistic CRC screening in China as supplementary exams. Additional research are wanted to confirm and enhance the grounded theoretical mannequin developed on this examine, and apply the theoretical outcomes into the real-world screening practices.
Knowledge availability assertion
The uncooked knowledge supporting the conclusions of this text will probably be made accessible by the authors, with out undue reservation.
Writer contributions
WX conceived and designed the examine. WW, YC, and MCW made substantial contributions to the examine design. WW drafted the manuscript. WW and ST contributed to knowledge assortment and knowledge sorting. ST and JH contributed to knowledge evaluation. All authors contributed to the article and authorised the submitted model.
Funding
This examine was supported by the Well being Fee of Pudong New Space of Shanghai (no. PW2019A-5).
Acknowledgments
We thank the specialists taking part the qualitative interview.
Battle of curiosity
The authors declare that the analysis was carried out within the absence of any industrial or monetary relationships that might be construed as a possible battle of curiosity.
Writer’s be aware
All claims expressed on this article are solely these of the authors and don’t essentially symbolize these of their affiliated organizations, or these of the writer, the editors and the reviewers. Any product which may be evaluated on this article, or declare which may be made by its producer, is just not assured or endorsed by the writer.
Abbreviations
BMI, physique mass index; CMS, facilities for medicare and medicaid providers; CDC, facilities for illness prevention and management; CRC, colorectal most cancers; FIT, fecal immunochemical check; gFOBT, guaiac fecal occult blood check; mSEPT9, methylated SEPT9 DNA plasma assay; mt-sDNA, multi-target stool DNA check; RA, threat evaluation.
References
1. Lin, JS, Perdue, LA, Henrikson, NB, Bean, SI, and Blasi, PR. Screening for colorectal Most cancers: up to date proof report and systematic overview for the US preventive providers process pressure. JAMA. (2021) 325:1978–97. doi: 10.1001/jama.2021.4417
2. Benard, F, Barkun, AN, Martel, M, and von Renteln, D. Systematic overview of colorectal most cancers screening tips for average-risk adults: summarizing the present world suggestions. World J Gastroenterol. (2018) 24:124–38. doi: 10.3748/wjg.v24.i1.124
PubMed Summary | Crossref Full Textual content | Google Scholar
3. Navarro, M, Nicolas, A, Ferrandez, A, and Lanas, A. Colorectal most cancers inhabitants screening applications worldwide in 2016: an replace. World J Gastroenterol. (2017) 23:3632–42. doi: 10.3748/wjg.v23.i20.3632
PubMed Summary | Crossref Full Textual content | Google Scholar
4. Schreuders, EH, Ruco, A, Rabeneck, L, Schoen, RE, Sung, JJ, Younger, GP, et al. Colorectal most cancers screening: a world overview of current programmes. Intestine. (2015) 64:1637–49. doi: 10.1136/gutjnl-2014-309086
PubMed Summary | Crossref Full Textual content | Google Scholar
5. Sung, JJ, Ng, SC, Chan, FK, Chiu, HM, Kim, HS, Matsuda, T, et al. An up to date Asia Pacific consensus suggestions on colorectal most cancers screening. Intestine. (2015) 64:121–32. doi: 10.1136/gutjnl-2013-306503
PubMed Summary | Crossref Full Textual content | Google Scholar
6. Dong, ZW
. Tips of most cancers screening, early detection and early remedy of China. 1st ed. Peking: Peking College Medical Press (2005).
7. Ye, D, Huang, Q, Li, Q, Jiang, X, Mamat, M, Tang, M, et al. Comparative analysis of preliminary screening strategies for colorectal Most cancers in a mass program. Dig Dis Sci. (2017) 62:2532–41. doi: 10.1007/s10620-017-4648-1
8. Gong, Y, Peng, P, Bao, P, Zhong, W, Shi, Y, Gu, Ok, et al. The implementation and first-round outcomes of a community-based colorectal Most cancers screening program in Shanghai. China Oncologist. (2018) 23:928–35. doi: 10.1634/theoncologist.2017-0451
PubMed Summary | Crossref Full Textual content | Google Scholar
9. Liao, Y, Li, S, Chen, C, He, X, Lin, F, Wang, J, et al. Screening for colorectal most cancers in Tianhe, Guangzhou: outcomes of mixing fecal immunochemical exams and threat elements for choosing sufferers requiring colonoscopy. Gastroenterol Rep (Oxf). (2018) 6:132–6. doi: 10.1093/gastro/gox030
PubMed Summary | Crossref Full Textual content | Google Scholar
10. Zhang, M, Zhao, L, Zhang, Y, Jing, H, Wei, L, Li, Z, et al. Colorectal Most cancers screening with excessive risk-factor questionnaire and fecal immunochemical exams amongst 5, 947, 986 asymptomatic inhabitants: a population-based examine. Entrance Oncol. (2022) 12:893183. doi: 10.3389/fonc.2022.893183
PubMed Summary | Crossref Full Textual content | Google Scholar
11. Meng, W, Cai, SR, Zhou, L, Dong, Q, Zheng, S, and Zhang, SZ. Efficiency worth of excessive threat elements in colorectal most cancers screening in China. World J Gastroenterol. (2009) 15:6111–6. doi: 10.3748/wjg.15.6111
PubMed Summary | Crossref Full Textual content | Google Scholar
12. Chen, H, Li, N, Ren, J, Feng, X, Lyu, Z, Wei, L, et al. Participation and yield of a population-based colorectal most cancers screening programme in China. Intestine. (2019) 68:1450–7. doi: 10.1136/gutjnl-2018-317124
PubMed Summary | Crossref Full Textual content | Google Scholar
13. Zheng, S, Chen, Ok, Liu, X, Ma, X, Yu, H, Chen, Ok, et al. Cluster randomization trial of sequence mass screening for colorectal most cancers. Dis Colon Rectum. (2003) 46:51–8. doi: 10.1007/s10350-004-6496-2
PubMed Summary | Crossref Full Textual content | Google Scholar
14. Wu, WM, Wang, Y, Jiang, HR, Yang, C, Li, XQ, Yan, B, et al. Colorectal Most cancers screening modalities in Chinese language inhabitants: follow and classes in Pudong new space of Shanghai, China. Entrance Oncol. (2019) 9:399. doi: 10.3389/fonc.2019.00399
PubMed Summary | Crossref Full Textual content | Google Scholar
15. Wu, W, Huang, J, Yang, Y, Gu, Ok, Luu, HN, Tan, S, et al. Adherence to colonoscopy in cascade screening of colorectal most cancers: a scientific overview and meta-analysis. J Gastroenterol Hepatol. (2022) 37:620–31. doi: 10.1111/jgh.15762
PubMed Summary | Crossref Full Textual content | Google Scholar
16. Money, BD, Fleisher, MR, Fern, S, Rajan, E, Haithcock, R, Kastenberg, DM, et al. Multicentre, potential, randomised examine evaluating the diagnostic yield of colon capsule endoscopy versus CT colonography in a screening inhabitants (the TOPAZ examine). Intestine. (2021) 70:2115–22. doi: 10.1136/gutjnl-2020-322578
PubMed Summary | Crossref Full Textual content | Google Scholar
17. Davidson, KW, Barry, MJ, Mangione, CM, Cabana, M, Caughey, AB, Davis, EM, et al. Screening for colorectal Most cancers: US preventive providers process pressure advice assertion. JAMA. (2021) 325:1965–77. doi: 10.1001/jama.2021.6238
PubMed Summary | Crossref Full Textual content | Google Scholar
18. Bibbins-Domingo, Ok, Grossman, DC, Curry, SJ, Davidson, KW, Epling, JW Jr, Garcia, FAR, et al. Screening for colorectal Most cancers: US preventive providers process pressure advice assertion. JAMA. (2016) 315:2564–75. doi: 10.1001/jama.2016.5989
PubMed Summary | Crossref Full Textual content | Google Scholar
19. Corbin, JM, and Strauss, A. Grounded idea analysis: procedures, canons, and evaluative standards. Qual Sociol. (1990) 13:3–21. doi: 10.1007/BF00988593
20. Starks, H, and Trinidad, SB. Select your methodology: a comparability of phenomenology, discourse evaluation, and grounded idea. Qual Well being Res. (2007) 17:1372–80. doi: 10.1177/1049732307307031
PubMed Summary | Crossref Full Textual content | Google Scholar
21. Tong, A, Sainsbury, P, and Craig, J. Consolidated standards for reporting qualitative analysis (COREQ): a 32-item guidelines for interviews and focus teams. Int J Qual Well being Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
PubMed Summary | Crossref Full Textual content | Google Scholar
22. World Medical Affiliation declaration of Helsinki
. Suggestions guiding physicians in biomedical analysis involving human topics. JAMA. (1997) 277:925–6. doi: 10.1001/jama.277.11.925
23. Damschroder, LJ, Aron, DC, Keith, RE, Kirsh, SR, Alexander, JA, and Lowery, JC. Fostering implementation of well being providers analysis findings into follow: a consolidated framework for advancing implementation science. Implement Sci. (2009) 4:50. doi: 10.1186/1748-5908-4-50
PubMed Summary | Crossref Full Textual content | Google Scholar
24. Kirk, MA, Kelley, C, Yankey, N, Birken, SA, Abadie, B, and Damschroder, L. A scientific overview of using the consolidated framework for implementation analysis. Implement Sci. (2016) 11:72. doi: 10.1186/s13012-016-0437-z
PubMed Summary | Crossref Full Textual content | Google Scholar
25. Cenin, D, Li, P, Wang, J, de Jonge, L, Yan, B, Tao, S, et al. Optimising colorectal most cancers screening in Shanghai, China: a modelling examine. BMJ Open. (2022) 12:e048156. doi: 10.1136/bmjopen-2020-048156
PubMed Summary | Crossref Full Textual content | Google Scholar
26. Peng, BJ, Cao, CY, Li, W, Zhou, YJ, Zhang, Y, Nie, YQ, et al. Diagnostic efficiency of intestinal Fusobacterium nucleatum in colorectal Most cancers: a Meta-analysis. Chin Med J. (2018) 131:1349–56. doi: 10.4103/0366-6999.232814
PubMed Summary | Crossref Full Textual content | Google Scholar
27. Lee, JK, Liles, EG, Bent, S, Levin, TR, and Corley, DA. Accuracy of fecal immunochemical exams for colorectal most cancers: systematic overview and meta-analysis. Ann Intern Med. (2014) 160:171. doi: 10.7326/m13-1484
PubMed Summary | Crossref Full Textual content | Google Scholar
28. Peterse, EFP, Meester, RGS, de Jonge, L, Omidvari, AH, Alarid-Escudero, F, Knudsen, AB, et al. Evaluating the cost-effectiveness of revolutionary colorectal Most cancers screening exams. J Natl Most cancers Inst. (2021) 113:154–61. doi: 10.1093/jnci/djaa103
PubMed Summary | Crossref Full Textual content | Google Scholar
29. Cai, SR, Huang, YQ, Zhang, SZ, Li, QR, Ma, XY, and Zheng, S. Results of subitems within the colorectal most cancers screening protocol on the Chinese language colorectal most cancers screening program: an evaluation based mostly on pure group screening outcomes. BMC Most cancers. (2019) 19:47. doi: 10.1186/s12885-018-5191-y
PubMed Summary | Crossref Full Textual content | Google Scholar
30. Yau TOTang, CM, Harriss, EK, Dickins, B, and Polytarchou, C. Faecal microRNAs as a non-invasive instrument within the analysis of colonic adenomas and colorectal most cancers: a meta-analysis. Sci Rep. (2019) 9:9491. doi: 10.1038/s41598-019-45570-9
PubMed Summary | Crossref Full Textual content | Google Scholar
31. Gachabayov, M, Lebovics, E, Rojas, A, Felsenreich, DM, Latifi, R, and Bergamaschi, R. Efficiency analysis of stool DNA methylation exams in colorectal most cancers screening: a scientific overview and meta-analysis. Shade Dis. (2021) 23:1030–42. doi: 10.1111/codi.15521
PubMed Summary | Crossref Full Textual content | Google Scholar
32. Nationwide Most cancers Heart, China
. Skilled Group of the Growth of China guideline for the screening, early detection and early remedy of colorectal Most cancers. [China guideline for the screening, early detection and early treatment of colorectal cancer (2020, Beijing)]. Zhonghua Zhong Liu Za Zhi. (2021) 43:16–38. doi: 10.3760/cma.j.cn112152-20210105-00010
33. Pecere, S, Senore, C, Hassan, C, Riggi, E, Segnan, N, Pennazio, M, et al. Accuracy of colon capsule endoscopy for superior neoplasia. Gastrointest Endosc. (2020) 91:406–414.e1. doi: 10.1016/j.gie.2019.09.041
PubMed Summary | Crossref Full Textual content | Google Scholar
34. Hassan, C, Zullo, A, Winn, S, and Morini, S. Price-effectiveness of capsule endoscopy in screening for colorectal most cancers. Endoscopy. (2008) 40:414–21. doi: 10.1055/s-2007-995565
PubMed Summary | Crossref Full Textual content | Google Scholar
35. Zauber, AG, Lansdorp-Vogelaar, I, Knudsen, AB, Wilschut, J, van Ballegooijen, M, and Kuntz, KM. Evaluating check methods for colorectal most cancers screening: a choice evaluation for the U.S. preventive providers process pressure. Ann Intern Med. (2008) 149:659–69. doi: 10.7326/0003-4819-149-9-200811040-00244
PubMed Summary | Crossref Full Textual content | Google Scholar
36. Wong, CK, Lam, CL, Wan, YF, and Fong, DY. Price-effectiveness simulation and evaluation of colorectal most cancers screening in Hong Kong Chinese language inhabitants: comparability amongst colonoscopy, guaiac and immunologic fecal occult blood testing. BMC Most cancers. (2015) 15:705. doi: 10.1186/s12885-015-1730-y
PubMed Summary | Crossref Full Textual content | Google Scholar
37. Wang, H, Ye, H, and Liu, L. Establishing massive knowledge prevention and management mannequin for public well being emergencies in China: a grounded idea examine. Entrance Public Well being. (2023) 11:1112547. doi: 10.3389/fpubh.2023.1112547
PubMed Summary | Crossref Full Textual content | Google Scholar
38. Chiu, HM, Chen, SLS, Yen, AMF, Chiu, SYH, Fann, JCY, Lee, YC, et al. Effectiveness of fecal immunochemical testing in lowering colorectal most cancers mortality from the a million Taiwanese screening program. Most cancers. (2015) 121:3221–9. doi: 10.1002/cncr.29462
PubMed Summary | Crossref Full Textual content | Google Scholar
40. Hassan, C, Giorgi Rossi, P, Camilloni, L, Rex, DK, Jimenez-Cendales, B, Ferroni, E, et al. Meta-analysis: adherence to colorectal most cancers screening and the detection charge for superior neoplasia, based on the kind of screening check. Aliment Pharmacol Ther. (2012) 36:929–40. doi: 10.1111/apt.12071
41. Lin, G, Feng, Z, Liu, H, Li, Y, Nie, Y, Liang, Y, et al. Mass screening for colorectal most cancers in a inhabitants of two million older adults in Guangzhou, China. Sci Rep. (2019) 9:10424. doi: 10.1038/s41598-019-46670-2
PubMed Summary | Crossref Full Textual content | Google Scholar
42. Miles, A, Rodrigues, V, and Sevdalis, N. The impact of details about false adverse and false optimistic charges on folks’s attitudes in the direction of colorectal most cancers screening utilizing faecal occult blood testing (FOBt). Affected person Educ Couns. (2013) 93:342–9. doi: 10.1016/j.pec.2013.06.010
PubMed Summary | Crossref Full Textual content | Google Scholar
43. Kaminski, MF, Robertson, DJ, Senore, C, and Rex, DK. Optimizing the standard of colorectal Most cancers screening worldwide. Gastroenterology. (2020) 158:404–17. doi: 10.1053/j.gastro.2019.11.026
PubMed Summary | Crossref Full Textual content | Google Scholar
44. Schreuders, EH, Grobbee, EJ, Nieuwenburg, SAV, Kapidzic, A, van Roon, AHC, van Vuuren, AJ, et al. A number of rounds of 1 pattern versus two pattern faecal immunochemical test-based colorectal most cancers screening: a population-based examine. Lancet Gastroenterol Hepatol. (2019) 4:622–31. doi: 10.1016/S2468-1253(19)30176-1
PubMed Summary | Crossref Full Textual content | Google Scholar
45. Peng, L, Weigl, Ok, Boakye, D, and Brenner, H. Threat scores for predicting superior colorectal neoplasia within the average-risk inhabitants: a scientific overview and Meta-analysis. Am J Gastroenterol. (2018) 113:1788–800. doi: 10.1038/s41395-018-0209-2
PubMed Summary | Crossref Full Textual content | Google Scholar
46. Williams, TG, Cubiella, J, Griffin, SJ, Walter, FM, and Usher-Smith, JA. Threat prediction fashions for colorectal most cancers in folks with signs: a scientific overview. BMC Gastroenterol. (2016) 16:63. doi: 10.1186/s12876-016-0475-7
PubMed Summary | Crossref Full Textual content | Google Scholar
47. Li, J, Li, QL, Xue, F, Yu, LL, and Ma, WL. Software of Faecal occult blood testing and questionnaire threat evaluation in inhabitants screening for colorectal Most cancers. China Most cancers. (2015) 24:385–9. doi: 10.11735/j.issn.1004-0242.2015.05.A008
48. Spada, C, Hassan, C, Bellini, D, Burling, D, Cappello, G, Carretero, C, et al. Imaging alternate options to colonoscopy: CT colonography and colon capsule. European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastrointestinal and Stomach Radiology (ESGAR) guideline – replace 2020. Eur Radiol. (2021) 31:2967–82. doi: 10.1007/s00330-020-07413-4
{kind=link}