
1 Introduction
Hypoxia in prostate most cancers (PCa) has been associated to radiation remedy resistance and metastatic illness (1–3). Thus, hypoxia evaluation at prognosis is of nice curiosity for affected person stratification and remedy selections. On condition that MRI is the primary imaging modality in PCa sufferers and broadly accessible in trendy hospitals, the consideration of MRI biomarkers emerges as a gorgeous instrument for remedy personalization. A promising strategy, utilizing diffusion-weighted photographs (DWI) associated to oxygen consumption and provide, was developed by Hompland et al. (4). This mannequin, referred to as Consumption and Provide primarily based Hypoxia (CSH) imaging, depends on obvious diffusion coefficient (ADC) and fractional blood quantity (fBV) maps and its utility to PCa sufferers was primarily based on the underlying assumption that the estimated ADC is linked to oxygen consumption whereas fBV is linked to oxygen provide.
The CSH mannequin was skilled utilizing DWI knowledge of PCa sufferers who acquired a hypoxia marker (pimonidazole) administration previous to prostatectomy as a floor fact to seek out the optimum mixture of ADC and fBV representing hypoxia. In a separate check cohort, the hypoxia fraction (HFDWI) of the index lesion confirmed a strong correlation to hypoxia estimated from pimonidazole staining of the surgical specimen. Consequently, the CSH mannequin seems as a promising non-invasive instrument for hypoxia evaluation, providing potential for personalised remedy selections. Certainly this strategy gave the impression to be fairly profitable for correlating the HFDWI to pimonidazole-derived hypoxia in cancers equivalent to breast and cervix (4–6).
To use such a mannequin extra broadly in medical observe, exterior validation is important. A primary hurdle is the potential variability in quantitative MRI parameters between scanners and facilities (7, 8). Right here we suggest a calibration methodology by scaling the quantitative MRI parameters in matched cohorts of sufferers.
A second hurdle for validation of HFDWI in relation to true hypoxia in prostate most cancers is that it depends on the supply of pimonidazole staining. Within the absence of pimonidazole stained specimen, we will make use of the established associations between hypoxia and pathological Grade Group (pGG), in addition to Tstage (2, 4). Subsequently, on this examine we intention to check the affiliation between HFDWI and pGG and pTstage in a cohort of sufferers who acquired a prostatectomy on the Netherlands Most cancers Institute (NKI) and evaluate these associations with these initially obtained by Hompland et al (4).
2 Supplies and strategies
2.1 Cohort description
The unique dataset from Oslo College Hospital consisted of 106 sufferers enrolled into the FuncProst examine (NTC01464216) (4). For the exterior dataset, males with biopsy-proven prostate most cancers and pre-operative MRI, who underwent radical prostatectomy between January 2010 and December 2020, had been retrospectively included after approval of the institutional evaluation board (IRBd21-108) on the NKI. Exclusion standards had been males with prior transurethral resection of the prostate, incomplete or technically poor-quality MRI or incomplete pathological specimens. A complete of 291 sufferers had been subjected to additional evaluation.
2.2 MRI acquisition and knowledge evaluation of the NKI cohort
MRI knowledge within the NKI cohort had been acquired utilizing principally a 3T scanner (Achieva [n=164], Achieva dStream [n=103] and Ingenia [n=21], Philips Healthcare, Greatest, the Netherlands). The MRI examination consisted of T2-weighted (T2w), DWI and a separate excessive b-value DWI acquisition (b= 1400 or 2000 s/mm2). Axial T2-weighted (T2w) turbo spin-echo photographs had been acquired (Repetition time = [2175 – 10233 ms], Echo time = [110 – 130 ms]) with a field-of-view from 140 mm x 140 mm to 284 mm x 284 mm and slice thickness of two.5 to 4 mm. DWI knowledge had been acquired with single-shot echo planar imaging sequences with b-values of 0, 200, 800 or 0,50,300,800 s/mm2. An in depth comparability of DWI acquisition parameters between facilities will be present in Supplementary Desk S1.
ADC and fBV maps had been calculated utilizing an intravoxel incoherent movement mannequin with a segmented match strategy (9) . Particulars of this evaluation will be present in Supplementary Evaluation.
Tumor delineations on MR photographs (T2w, ADC and excessive b-value DWI scans) had been carried out by two observers (M.D.C. and M.F.S., each 1-2 years’ studying expertise) blinded to the pathological floor fact. If required, consensus was reached after dialogue with an skilled radiologist (I.G.S. 13 years of expertise). Histological analysis was carried out by a pathologist (M.A.S.G., 10 years of expertise) utilizing SlideScore software program [https://www.slidescore.com/]. Lesions bigger than 3 mm had been graded in keeping with the 2019 Worldwide Society of Urological Pathology suggestions (10). Staging was carried out in accordance the TNM classification tips (11). For sufferers with a number of lesions, solely the lesion with the best pGG was used.
2.3 CSH mannequin and calculation of hypoxia fraction
Beforehand, Hompland et al (4) confirmed that the discrimination of hypoxic and non-hypoxic areas might be approximated to a linear curve expressed as Equation (1)
the place ADC0 and fBV0 are the intersections with the ADC and fBV axes on a pixel-level plot (Determine 1). ADC0 = 0.79 x 10-3 mm2/s and fBV0 = 0.43 a.u. had been the intercepts for which HFDWI had the best correlation with the hypoxia rating from pimonidazole staining (HSpimo) within the Oslo cohort.
Determine 1 Instance of the CSH mannequin utility on a lesion (purple contour) of the NKI cohort. HL, hypoxia degree (pixel-level); HFDWI, hypoxia fraction (lesion-level).
As variations in acquisition and evaluation protocols between the 2 facilities had been current (Supplementary Desk S1), particularly within the numbers of b-values used, median scaling of the ADC and fBV distributions was utilized. Nonetheless, to ensure that variations in medical traits weren’t additionally affecting these variations, the cohorts had been first matched primarily based on medical traits. For this goal, propensity rating matching was used and 106 sufferers from the NKI cohort had been chosen to clinically match the 106 sufferers dataset from the unique establishment (utilizing pGG and pTstage as covariates). The choice to prioritize matching primarily based on pGG and pTstage was pushed by their recognized affiliation with hypoxia (2, 4). When a number of lesions had been current, the affected person’s pGG corresponded to the lesion with the best pGG. The R library MatchIt package deal (12) was used with optimum matching methodology, logistic regression distances and ‘Common Remedy Impact on the Management’ estimand (ATC), the place solely NKI sufferers are allowed to be dropped throughout the matching course of, whereas sustaining Oslo variety of sufferers mounted. This produced the very best match primarily based on customary imply variations.
For median scaling, the ADC and fBV voxel intensities distributions from all lesions of the matched NKI cohort had been scaled in the direction of the distributions of the Oslo dataset by multiplying them with the calculated scaled components [FADC and FfBV, Equation (2)].
As soon as the scaling was carried out for the medical matched set of sufferers, the HFDWI metric was computed for every lesion utilizing the ADC0 and fBV0 intercepts (Determine 1).
2.4 Hypoxia fraction validation and utility
Absolutely the HFDWI values had been investigated by evaluating the distributions inside every pGG (low: pGG < 3 and excessive: pGG ≥ 3) and every pTstage group between facilities. This comparability aimed to validate the consistency of HFDWI values between the 2 facilities for every particular medical subgroup.
Furthermore, HFDWI variations had been examined between sufferers with low versus excessive pGG, and pTstage = 2 versus pTstage = 3 within the matched NKI cohort. These variations had been then in comparison with the corresponding variations noticed within the Oslo cohort. T-tests or Mann-Whitney assessments (p< 0.05) had been used for these comparisons, relying on normality and homogeneity (i.e. with equal variances) assessed by the Shapiro-Wilk check and Levene’s check, respectively.
Lastly, the CSH mannequin was utilized to the complete NKI cohort (n=319 lesions from 291 sufferers) to research the HFDWI relation and correlation throughout particular person pGG teams utilizing a Kruskal-Wallis (p< 0.05) and the Pearson correlation coefficient assessments (ρ, p< 0.05). All analyses had been carried out utilizing Python v3.7.
3 Outcomes
The Oslo cohort was properly balanced by way of high and low pGG whereas general dominated by pTstage 3 sufferers. In distinction, the complete NKI cohort was dominated by low pGG and pTstage 2 sufferers. After propensity rating matching, the matched NKI cohort had comparable affected person traits because the Oslo cohort (Desk 1).
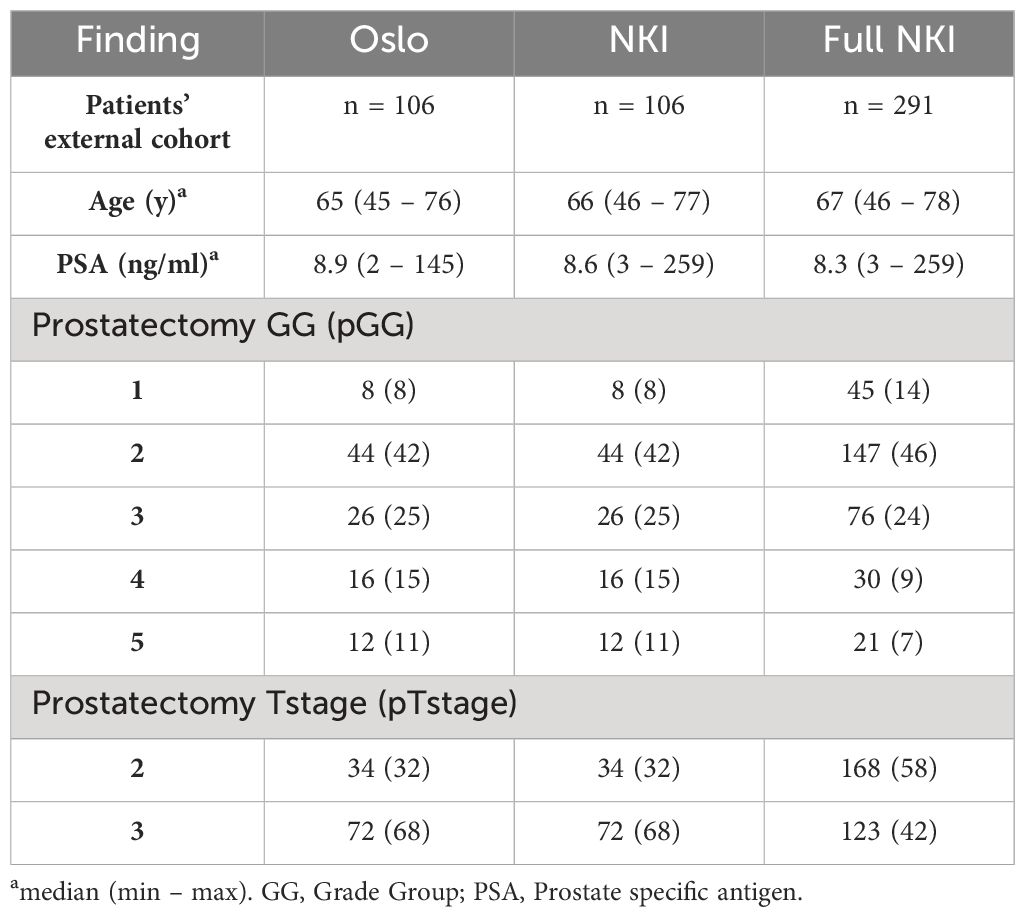
Desk 1 Affected person demographics and tumor traits for the unique cohort (Oslo), the matched exterior cohort (NKI, pGG of the index lesion) and the complete exterior cohort (Full NKI, with pGG info for all 319 lesions in 291 sufferers).
With comparable affected person traits between the 2 cohorts we anticipate variations in ADC and fBV values to principally replicate variations within the imaging acquisitions and MRI equipment.
Previous to scaling, the matched NKI dataset confirmed barely greater ADC values (median (IQR) was 0.84 (0.41) x10-3 mm/s2) in comparison with the Oslo cohort (0.70 (0.26) x10-3 mm/s2) and barely decrease fBV values (NKI: 0.08 (0.15) a.u. vs Oslo: 0.12 (0.11) a.u.) (Supplementary Determine S1). The obtained scaling components FADC and FfBV had been 0.83 and 1.54, respectively.
No statistically important variations had been noticed when evaluating the matched NKI distributions of absolute HFDWI values to the Oslo cohort for every particular pGG and pTstage subgroup (Determine 2, p(pGG<3) = 0.3, p(pGG>=3) = 0.8, p(pTstage=2) = 0.1, p(pTstage=3) = 0.4). HFDWI median values for Oslo had been 0.11 vs 0.27 for high and low pGG, and 0.08 vs 0.26 for pTstage = 2 and pTstage = 3. Median values for NKI had been 0.17 vs 0.24 and 0.17 vs 0.22 for pGG and pTstage teams, respectively. The affiliation between HFDWI and pGG and pTstage was constant between the Oslo and the matched NKI dataset (Determine 3): each confirmed that greater HFDWI values had been related to greater pGG (Oslo p<0.001, NKI p=0.004) and pTstage teams (Oslo p<0.001, NKI p=0.03). Moreover, important variations had been noticed amongst all pGG teams within the full NKI cohort (Determine 4, p< 0.001), along with a major constructive correlation (ρ = 0.41, p< 0.001).
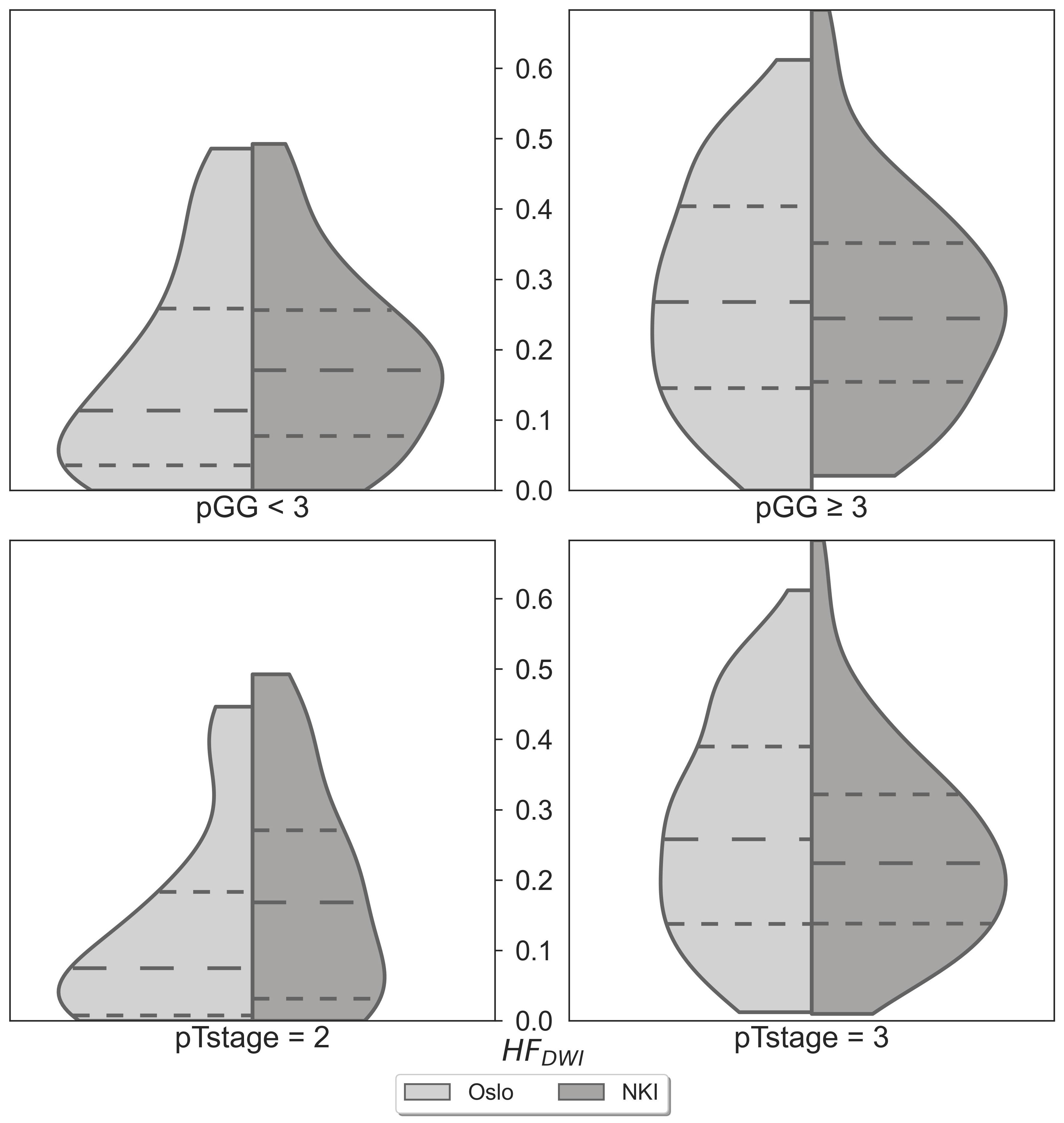
Determine 2 HFDWI comparability between the Oslo (n=106) and NKI (n=106) datasets for particular pGG and pTstage sub-groups.
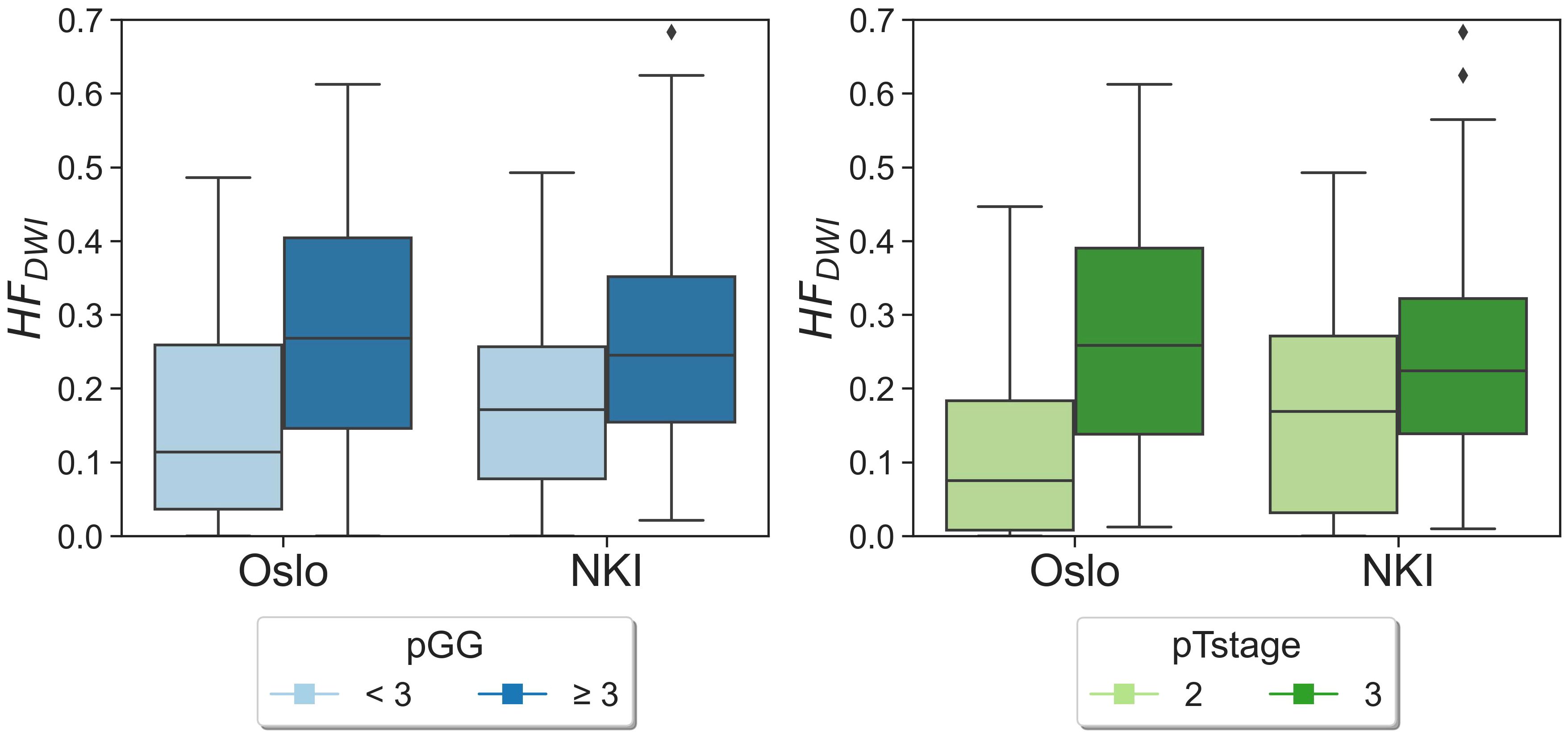
Determine 3 HFDWI distributions for pGG and pTstage teams for each Oslo and NKI datasets. Diamond symbols characterize outliers of the distributions.
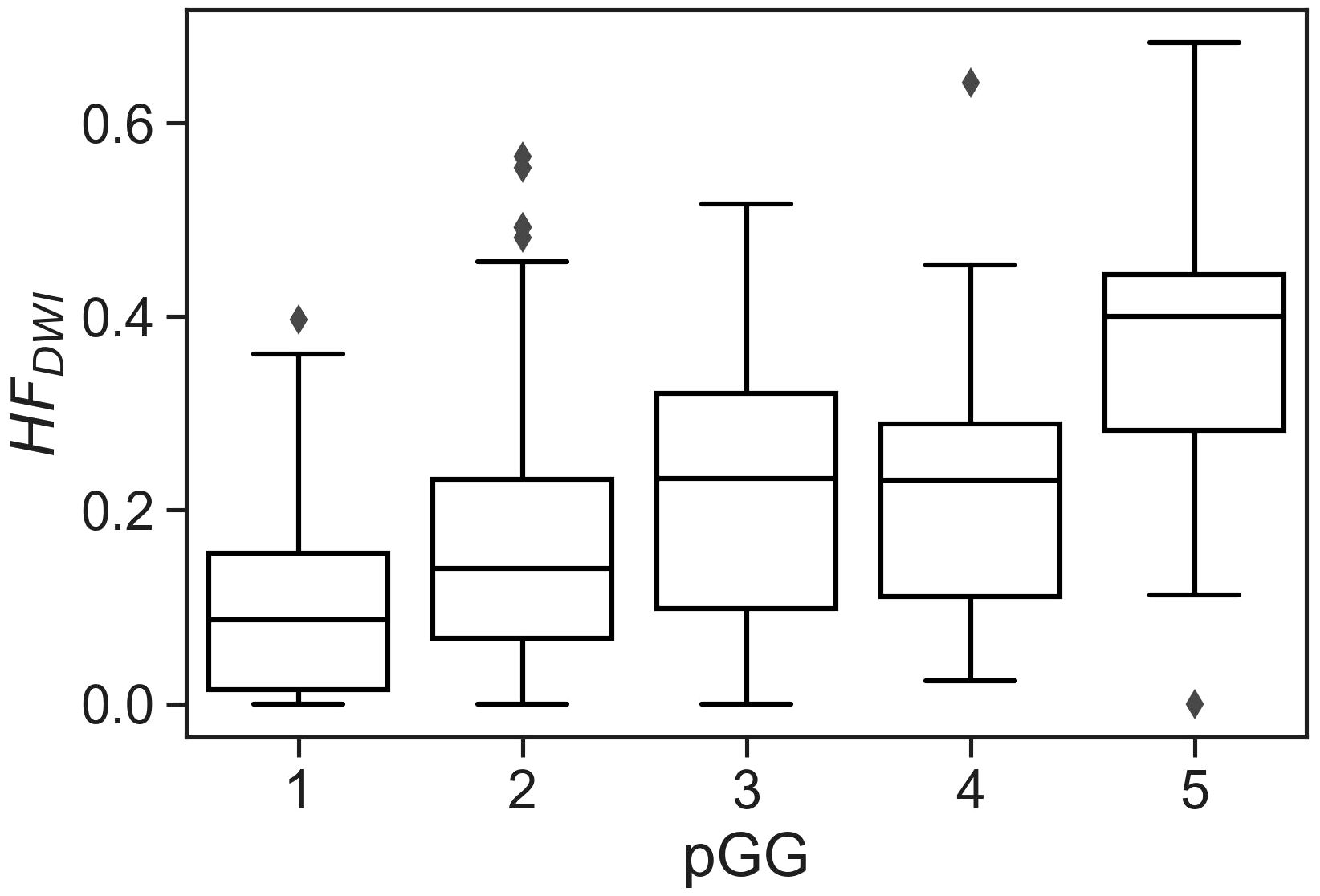
Determine 4 CSH mannequin utilized to the complete NKI cohort (319 lesions from 291 sufferers) exhibiting the correlation between hypoxia fraction with pGG individually. Kruskal-Wallis p< 0.001 signifies important variations amongst teams.
4 Dialogue
The intention of this examine was to independently validate the CSH mannequin in prostate most cancers by evaluating the HFDWI affiliation with pGG and pTstage in an unbiased exterior prostatectomy cohort.
After clinically matching and scaling, the HFDWI within the NKI dataset exhibited comparable associations with the pGG and pTstage teams as noticed within the Oslo dataset. In settlement with Hompland et al. (4), a affected person with a excessive HFDWI within the NKI cohort was more likely to exhibit extra aggressive traits, equivalent to the next pTstage or pGG, compared to a affected person with a decrease HFDWI. Moreover, the HFDWI absolute values obtained within the NKI dataset had been similar to these of the Oslo dataset for each pGG and pTstage subgroups. Whereas pimonidazole staining was unavailable within the NKI cohort, this similarity means that HFdwi can also point out hypoxia within the NKI cohort.
Previous to scaling, the ADC and fBV distributions of the Oslo and NKI datasets weren’t very completely different (Supplementary Determine S1). That is an attention-grabbing remark as technical variations (together with variations in vendor, sequence protocols, and knowledge evaluation strategies) had been current between the 2 cohorts. Nonetheless, for future functions of the CSH mannequin in different datasets, ADC and fBV distributions must be rigorously in contrast with the Oslo knowledge for an correct use of the hypoxia metric. To permit different institutes to use this methodology and decide scaling parameters for his or her cohort, all voxel values of ADC and fBV for the Oslo dataset and NKI matched dataset will be present in Supplementary Information S1, Information S2 respectively. The framework for the CSH mannequin utility between completely different cohorts offered on this examine affords a helpful template for transferring different quantitative MRI biomarkers between completely different cohorts.
For example, the mannequin was utilized to the complete accessible NKI cohort of 291 sufferers, exhibiting constant outcomes for particular person pGG classes. The constructive correlation noticed between HFDWI and the person pGG classes probably positions the CSH-model as a non-invasive methodology to establish or classify sufferers into particular pGG teams.
A limitation of this examine is the dearth of pimonidazole staining to biologically validate the HFDWI metric in an exterior cohort. Nonetheless, we confirmed that correlations between HFDWI and measures of tumor aggressiveness and unfold might be replicated in an exterior dataset.
MRI has the potential to non-invasively assess hypoxia in prostate most cancers, proven by the present exterior validation of the connection between HFDWI and pGG/pTstage, beforehand proven by Hompland et al. (4). MRI could thereby be succesful in stratifying sufferers who’re at the next threat of worse medical outcomes, e.g. illness development or radiation resistance. Future analysis ought to deal with exterior validations throughout various medical settings to make sure the robustness and generalizability of the CSH mannequin.
5 Conclusion
The CSH mannequin exhibited enough robustness within the exterior cohort, suggesting a believable reflection of true hypoxia and enabling the usage of the HFDWI metric for additional analysis into PCa and hypoxia.
Information availability assertion
The unique contributions offered within the examine are included within the article/Supplementary Materials. Additional inquiries will be directed to the corresponding writer.
Ethics assertion
The research involving people had been permitted by the Netherlands Most cancers Institute – IRBd21-108. The research had been carried out in accordance with the native laws and institutional necessities. The ethics committee/institutional evaluation board waived the requirement of written knowledgeable consent for participation from the contributors or the contributors’ authorized guardians/subsequent of kin as a result of pursuant to nationwide laws previous to 25 Might 2018 (Decide-out) and Normal hospital knowledgeable consent was thought of.
Creator contributions
MF: Conceptualization, Information curation, Formal evaluation, Investigation, Methodology, Software program, Validation, Visualization, Writing – unique draft, Writing – evaluation & enhancing. TH: Conceptualization, Writing – evaluation & enhancing, Software program. M-DC: Information curation, Writing – evaluation & enhancing. HV: Writing – evaluation & enhancing. EB: Writing – evaluation & enhancing. MG: Information curation, Writing – evaluation & enhancing. HL: Writing – evaluation & enhancing. UV: Supervision, Writing – evaluation & enhancing. IS: Supervision, Writing – evaluation & enhancing. PV: Conceptualization, Methodology, Supervision, Writing – evaluation & enhancing.
Funding
The writer(s) declare monetary assist was acquired for the analysis, authorship, and/or publication of this text. This undertaking has been based by a KWF grant. Undertaking quantity: 12975.
Battle of curiosity
The authors declare that the analysis was carried out within the absence of any industrial or monetary relationships that might be construed as a possible battle of curiosity.
Writer’s observe
All claims expressed on this article are solely these of the authors and don’t essentially characterize these of their affiliated organizations, or these of the writer, the editors and the reviewers. Any product which may be evaluated on this article, or declare which may be made by its producer, will not be assured or endorsed by the writer.
Supplementary materials
The Supplementary Materials for this text will be discovered on-line at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1433197/full#supplementary-material
Footnotes
References
1. Milosevic M, Warde P, Ménard C, Chung P, Toi A, Ishkanian A, et al. Tumor hypoxia predicts biochemical failure following radiotherapy for clinically localized prostate most cancers. Clin Most cancers Res. (2012) 18:2108–14. doi: 10.1158/1078-0432.CCR-11-2711
PubMed Summary | CrossRef Full Textual content | Google Scholar
2. Ragnum HB, Vlatkovic L, Lie AK, Axcrona Okay, Julin CH, Frikstad KM, et al. The tumour hypoxia marker pimonidazole displays a transcriptional programme related to aggressive prostate most cancers. Br J Most cancers. (2015) 112:382–90. doi: 10.1038/bjc.2014.604
PubMed Summary | CrossRef Full Textual content | Google Scholar
3. Turaka A, Buyyounouski MK, Hanlon AL, Horwitz EM, Greenberg RE, Movsas B. Hypoxic prostate/muscle Po2 ratio predicts for final result in sufferers with localized prostate most cancers: long-term outcomes. Int J Radiat Oncol Biol Phys. (2012) 82:e433–e9. doi: 10.1016/j.ijrobp.2011.05.037
PubMed Summary | CrossRef Full Textual content | Google Scholar
4. Hompland T, Gap KH, Ragnum HB, Aarnes E-Okay, Vlatkovic L, Lie AK, et al. Mixed MR imaging of oxygen consumption and provide reveals tumor hypoxia and aggressiveness in prostate most cancers sufferers. Most cancers Res. (2018) 78:4774–85. doi: 10.1158/0008-5472.CAN-17-3806
PubMed Summary | CrossRef Full Textual content | Google Scholar
5. Hillestad T, Hompland T, Fjeldbo CS, Skingen VE, Salberg UB, Aarnes E-Okay, et al. MRI distinguishes tumor hypoxia ranges of various prognostic and organic significance in cervical most cancers. Most cancers Res. (2020) 80:3993–4003. doi: 10.1158/0008-5472.CAN-20-0950
PubMed Summary | CrossRef Full Textual content | Google Scholar
6. Mo T, Brandal SHB, Köhn-Luque A, Engebraaten O, Kristensen VN, Fleischer T, et al. Quantification of tumor hypoxia by means of unsupervised modelling of consumption and provide hypoxia MR imaging in breast most cancers. Cancers. (2022) 14:1326. doi: 10.3390/cancers14051326
PubMed Summary | CrossRef Full Textual content | Google Scholar
7. Shukla-Dave A, Obuchowski NA, Chenevert TL, Jambawalikar S, Schwartz LH, Malyarenko D, et al. Quantitative imaging biomarkers alliance (QIBA) suggestions for improved precision of DWI and DCE-MRI derived biomarkers in multicenter oncology trials. J Magnet Resonance Imaging. (2019) 49:e101–e21. doi: 10.1002/jmri.26518
8. Van Houdt PJ, Kallehauge JF, Tanderup Okay, Nout R, Zaletelj M, Tadic T, et al. Phantom-based high quality assurance for multicenter quantitative MRI in regionally superior cervical most cancers. Radiother Oncol. (2020) 153:114–21. doi: 10.1016/j.radonc.2020.09.013
PubMed Summary | CrossRef Full Textual content | Google Scholar
9. Kooreman ES, Van Houdt PJ, Keesman R, Van Pelt VWJ, Nowee ME, Pos F, et al. Every day intravoxel incoherent movement (IVIM) in prostate most cancers sufferers throughout MR-guided radiotherapy—A multicenter examine. Entrance Oncol. (2021) 11. doi: 10.3389/fonc.2021.705964
PubMed Summary | CrossRef Full Textual content | Google Scholar
10. van Leenders GJLH, van der Kwast TH, Grignon DJ, Evans AJ, Kristiansen G, Kweldam CF, et al. The 2019 worldwide society of urological pathology (ISUP) consensus convention on grading of prostatic carcinoma. Am J Surg Pathol. (2020) 44:e87–99. doi: 10.1097/PAS.0000000000001497
PubMed Summary | CrossRef Full Textual content | Google Scholar
11. Sobin LH GM, Wittekind C. TNM classification of Malignant tumours. seventh version. West Sussex, United Kingdom: Wiley Blackwell (2009).
{kind=link}